Review
Review

Affiliation:
Department of Educational Sciences, Section of Psychology, University of Catania, 95124 Catania, Italy
Email: graziellachiara.prezzavento@studium.unict.it
ORCID: https://orcid.org/0000-0002-0234-7011
Explor Asthma Allergy. 2024;2:97–110 DOI: https://doi.org/10.37349/eaa.2024.00032
Received: July 31, 2023 Accepted: January 15, 2024 Published: April 08, 2024
Academic Editor: Giorgio Walter Canonica, Humanitas University, Humanitas Research Hospital, Italy
The article belongs to the special issue Asthma and its Relationship with Psychological and Psychopathological Factors
Respiratory changes are often associated with anxiety disorders, particularly panic disorder (PD). Individuals experiencing PD are subjected to unexpected panic attacks, marked by overwhelming anxiety and fear, leading to a variety of autonomic and respiratory symptoms. PD patients have increased sensitivity to carbon dioxide (CO2). In response to respiratory stimulants like CO2, patients with PD tend to hyperventilate and panic, triggering the activation of an excessively reactive fear network. While their respiratory physiology may appear normal, the presence of subtle breathing abnormalities and other functions related to bodily homeostasis. This fear network, comprising the hippocampus, medial prefrontal cortex, amygdala, and its connections to the brainstem, seems to be hypersensitive in PD’s patients. This review aims to present a comprehensive overview of the current landscape on the link between PD and respiratory disorders. In July 2023 a literature search was undertaken for articles examining the relationship between PD, respiratory disorders, and psychological implications. Multiple databases were searched: PubMed, PubMed Central, PsycINFO, Web of Science, Elsevier Journal, Health & Medical Collection, and Springer. The analysis of six studies focused on the correlation between PD and asthma revealed important links between these two disorders. Anxiety and panic can have significant impacts on the manifestation and aggravation of asthma. Furthermore, the review indicates that psychological therapeutic approaches, in particular cognitive-behavioral therapy, may represent a valid intervention to improve clinical outcomes in patients suffering from both disorders. Future investigations in this field may help highlight new intervention strategies in the psychological area to help individuals with PD decrease concomitant asthma, significantly improving their quality of life.
Anxiety disorders, including panic disorder (PD) with or without agoraphobia, generalized anxiety disorder, social anxiety disorder, specific phobias, and separation anxiety disorder, are the most prevalent mental disorders in the 21st century and are associated with immense health care costs and a high burden of disease [1]. Among anxiety disorders, PD has the highest prevalence rates in the general population [2]. Individuals diagnosed with PD frequently experience distressing panic attacks (PAs), marked by sudden and unexpected episodes of intense fear and discomfort [3]. The psychophysiological manifestations encompass a wide range of somatic, physical, and cognitive aspects. Among them are sensations such as palpitations, excessive sweating, trembling, a feeling of breathlessness, a sense of choking, chest pain or discomfort, nausea, dizziness, chills or sudden heat sensations, paresthesia or numbness, a feeling of detachment from oneself (depersonalization) or a sense of detachment from the surroundings (derealization), as well as fears of losing control, going insane, or facing imminent death [4]. Numerous studies have delved into the connection between PD and the respiratory system, shedding light on intriguing findings [5]. Among patients with PD, respiratory abnormalities are frequently observed, signifying a potential link between the two [6]. Notably, individuals with PD exhibit distinct respiratory patterns during resting periods, characterized by elevated minute ventilation, lower levels of carbon dioxide (CO2) concentration in expired air, and irregular breathing [6]. These respiratory dysfunctions are believed to play a critical role in making individuals with PD more vulnerable to experiencing PAs. Such aberrations in respiratory function appear to be specific to PD and are not typically found in other anxiety disorders, such as social phobia or generalized anxiety disorder [7].
In a notable study conducted by Fullana et al. [8], which involved a large sample of 8,796 individuals from six European countries, 2,257 participants were identified as experiencing PA. These individuals were further categorized into two groups based on the presence or absence of shortness of breath during the PA episodes. The results revealed that the respiratory group, characterized by PAs accompanied by shortness of breath, accounted for a substantial 70% of the total cases. Notably, this respiratory group demonstrated a higher utilization of healthcare services compared to the non-respiratory group. The study also shed light on the lifetime prevalence of respiratory PAs, which was found to be 6.77% in the overall sample, compared to 3.14% in the non-respiratory group. These findings provide valuable insights into the prevalence and impact of respiratory symptoms during PAs, underscoring the significance of addressing this specific subgroup in clinical practice and research.
The etiology of PD remains a subject of ongoing investigation, with much yet to be fully comprehended. One prevailing perspective, the neuroanatomical hypothesis, posits that a complex interplay between genetic factors and environmental influences likely underlies the development of PD [9]. Research suggests that individuals with PD may manifest abnormalities in certain brain structures, experience altered neuronal processes, and encounter disrupted corticolimbic interactions during emotional processing [10]. Studies conducted on patients with symptomatic PD have revealed intriguing neurobiological findings [11]. Specifically, there have been observed reductions in midbrain serotonin transporter (5-HTT) and serotonin-1A (5-HT1A) receptor binding. These changes may indicate a compensatory mechanism aimed at enhancing serotonin (5-HT) neurotransmission, particularly in the dorsal periaqueductal gray-amygdala pathway. The goal of this compensatory process is likely to inhibit hyperactivity or spontaneous neuronal discharge in this brain region [11]. Moreover, patients with PD exhibit dysfunction in gamma-aminobutyric acid (GABA) receptors and/or altered concentrations of the neurotransmitter GABA in the brain. This suggests an intricate interplay between the serotonergic and GABAergic systems in the pathophysiology of PD. To address the symptoms of PD, therapeutic approaches have primarily focused on medications with anxiolytic properties. These include benzodiazepines, which potentiate GABA’s effects by modulating the function of GABA receptors, and selective 5-HT reuptake inhibitors (SSRIs), which increase the synaptic availability of 5-HT by blocking its reuptake into neurons [12].
Recent studies have delved into the association between insecure attachment and PD [13]. The attachment figure plays a crucial role in modulating the stress system, particularly in influencing the physiological responses of the child. This aspect holds particular relevance in the context of children with PD, where the intricate interplay between the attachment figure and the child’s stress system becomes a focal point [14]. The etiological explanation for PA from a psychological standpoint emphasizes the potential impact of insecure attachment during childhood as a risk factor for the development of anxiety disorders. When parents inconsistently or unresponsively react to a child’s distress, it can pave the way for the formation of insecure attachment patterns, ultimately contributing to the emergence of anxiety-related conditions later in life. These insecure attachment styles encompass avoidant behavior (detaching from caregiver figures), anxious-ambivalent behavior (excessively seeking attachment to caregiver figures and displaying anger upon rejection), and disorganized behavior (exhibiting inconsistent attachment behaviors). Notably, research by Cassidy et al. [13] demonstrated that individuals with PD are more likely to exhibit insecure attachment styles compared to control groups. In particular, ambivalent and avoidant attachment styles emerged as significant predictors of PD.
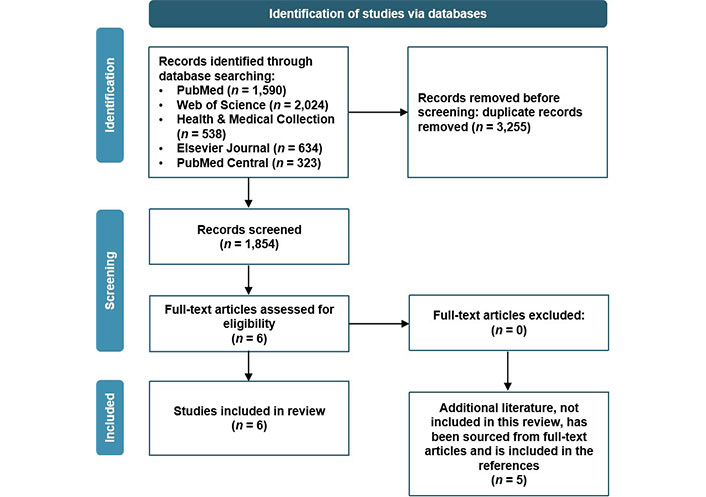
In July 2023, a series of searches was conducted using the search engines Summon [15] and Google Scholar [16] to gather relevant studies on the relationship between PDs and asthma. The search terms were selected to capture relevant studies related to the specific interventions and the target population. The number of results obtained from each database was recorded to assess the volume of literature available. PubMed, PubMed Central, Health & Medical Collection, Elsevier Journal, and Web of Science were used to identify relevant articles. The search terms were carefully selected to align with the objectives of the review.
In total, six papers were selected and analyzed from the searches [17–22]. The search process involved specific combinations of terms: “(PD) and (asthma)”; “(PA) and (asthma)”; “(respiratory disorders) or (PDs) and (anxiety)”. Duplicate papers were removed, and those not aligned with the themes were excluded.
This review includes the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram [23] to describe the research methodology and selection of articles included. Additional bibliography (not reported in the flow diagram) has been extrapolated from full-text articles and included as references [24–28].
Every article meeting the following criteria was included:
All studies and reviews published in indexed journals and indexed in PubMed, PubMed Central, Health & Medical Collection, Elsevier Journal, or Web of Science databases, related to PD in individuals with asthma.
Every article meeting the following criteria was excluded:
Studies related to PD in subjects without concomitant symptoms related to asthma.
All articles explore the association between anxiety disorders and respiratory disorders, without specifically focusing on PD and asthma.
Studies published in non-scientific or non-peer-reviewed sources.
In this literature review, a total of six full-text articles were included to analyze the correlation between PDs and respiratory disorders (Figure 1) [17–22].
The present review article provides a summary of six studies that explore the presence of prominent respiratory symptoms (i.e., dyspnea, feeling of choking, and breathlessness) during PAs to assess correlation with psychological factors. The studies included in this review are prospective studies, pilot studies, and research articles (Table 1). The studies were analyzed qualitatively, and the findings were synthesized to provide an overview of the current state of research in this area. The limitations of the studies and the implications for future research are also discussed.
Data extraction
| Author(s) | Year | Title | Study design | Focus | Sample (n) | Main results |
|---|---|---|---|---|---|---|
| Hasler et al. [17] | 2005 | Asthma and panic in young adults: a 20-year prospective community study | Prospective community study | Shed light on the dynamic interaction between asthma and panic, and uncover potential mechanisms underlying their comorbidity | 591 | Asthma predicted panic, whereas panic did not predict subsequent asthma activity. Smoking, early childhood anxiety, and a family history of allergies were important confounders of the asthma-panic association |
| Ross et al. [18] | 2005 | Cognitive-behavioral treatment combined with asthma education for adults with asthma and coexisting panic disorder | Randomized controlled trial (RCT) | Tested the efficacy of cognitive-behavioral therapy (CBT) treatment combined with an asthma education (AE) program for adults with asthma suffering from coexisting PD | 48 | CBT-AE program is capable of producing substantial and durable anti-panic and antianxiety treatment effects and led to substantial but non-sustained improvement in morning peak-flow expiratory rate and asthma-related quality of life |
| Lehrer et al. [19] | 2008 | Psychological treatment of comorbid asthma and panic disorder: a pilot study | Pilot study | Evaluate two protocols for treating adults with comorbid asthma and PD, which include elements of Barlow’s panic control therapy and several AE programs | 10 | Significant decreases in panic symptoms, clinically significant decreases in asthma symptoms, improvement in asthma quality of life, and maintenance of clinical stability in asthma. Albuterol use decreased significantly in the 14-session protocol and at a borderline level in the 8-session protocol, while the pulmonary function was maintained |
| Parry et al. [20] | 2012 | Cognitive behavioural intervention for adults with anxiety complications of asthma: prospective randomised trial | Prospective randomized trial | Verify if there is a reduction in asthma-specific fear after the cognitive-behavioral intervention compared with routine treatment | 94 | Significantly greater reduction in asthma-specific fear for people in the CBT group compared with controls. At 6 months after treatment the reduction in asthma-specific fear in the CBT group was increased and the difference between the treatment and control group was statistically significant |
| Bonnert et al. [21] | 2021 | Targeting excessive avoidance behavior to reduce anxiety related to asthma: a feasibility study of an exposure-based treatment delivered online | A feasibility study of an exposure-based treatment delivered online | Assess the feasibility and potential efficacy of the online CBT | 30 | CBT for avoidance behavior is a viable treatment for anxiety-related to asthma. CBT targeting avoidance behavior is effective in reducing catastrophizing about asthma (CAS). Additionally, all secondary outcomes, such as asthma control, avoidance behavior, fear of asthma symptoms, and quality of life, improve significantly with moderate to large effect sizes |
| Freire et al. [22] | 2013 | The panic disorder respiratory ratio: a dimensional approach to the respiratory subtype | Observational study | Determine whether the respiratory ratio is correlated with CO2-induced PAs and other clinical and demographic features | 91 | The respiratory ratio is correlated with CO2 sensitivity and there is a non-statistically significant trend toward a correlation with a family history of PD |
Asthma is a significant public health concern, and its prevalence has been on the rise in recent decades due to various environmental factors [24]. While the role of psychological factors in influencing asthma’s onset and progression has gained increasing recognition, one notable area of investigation is the potential association between asthma and panic. Several potential mechanisms may underlie the association between these disorders. Higher levels of anxiety may arise in individuals with asthma, which may lead to panic, mainly through fear conditioning triggered by dyspnea and respiratory receptor set-point disturbances [25]. In addition, some asthma medications may have anxiogenic properties, and anxiety may further exacerbate the use of asthma medications [26]. In addition, childhood stress has been associated with an increased risk of asthma and panic onset and recurrence [27]. Cross-sectional community-based studies have provided initial evidence of a relatively specific link between the prevalence of asthma and panic [28]. However, these studies have their limitations, such as varying definitions of panic and a lack of information on the temporal relationship between asthma and panic. To gain a deeper understanding of these mechanisms, long-term longitudinal studies are essential to examine potential causal relationships and the directionality of comorbid conditions.
A very interesting long-term longitudinal study is that of Hasler et al. [17], which explores the relationship between asthma and panic in a community sample of young adults. This study aims to shed light on the dynamic interaction between these two conditions and to uncover potential mechanisms underlying their comorbidity. The importance of this study lies in its focus on longitudinal associations, which offer valuable insights into the directionality and causal nature of the asthma-panic relationship. The study results reveal bidirectional associations between asthma and PD, indicating a complex and intertwined relationship. In particular, the authors conduct a comprehensive analysis of potential confounding factors and determinants that influence the asthma-panic association. Family history of allergy, smoking habit, and early childhood anxiety emerged as crucial factors influencing this comorbidity. The presence of shared etiologic factors, as well as potential genetic links, suggests a multifaceted origin for the co-occurrence of asthma and panic in young adults. The strength of this study lies in its community-based design, mitigating potential selection biases found in clinic-based investigations. The use of longitudinal data allows for a more nuanced understanding of the relationship between asthma and panic, building on the findings of prior longitudinal studies. Moreover, the reliable self-report data on asthma diagnosis, in combination with the extensive medication usage among participants, supports the robustness of the asthma data collected.
Comorbidity between asthma and PD is quite common and it is believed that the two pathologies interact with each other, increasing morbidity for each of them. This is due to the significant overlap of symptoms, such as breathlessness and tightness in the chest, which can lead to confusion and errors in self-care [29]. The recommended modes of self-treatment for the two pathologies may conflict, for example, exposure to body sensations for PD versus avoidance of asthma triggers. Symptomatological confusion can cause inappropriate, potentially dangerous treatments. Asthma can increase the risk of developing PD through various cognitive and behavioral mechanisms. Patients with PD may overreact to asthmatic symptoms and overuse asthma medications, such as albuterol, which may increase anxiety [30]. Hyperventilation, a common symptom of PD, can cause bronchospasm, and anxiety and stress can contribute to airway inflammation, increasing vulnerability to upper respiratory infections, which can trigger asthmatic exacerbations [31].
Increasing evidence that asthma and PD can exacerbate each other has led to a need for a combined treatment approach [32]. A study by Lehrer et al. [19] used CBT associated with AE, specifically combining elements of panic control therapy and asthma self-management programs, adapted for the group of patients with comorbidities. The pilot study was conducted to explore the effectiveness of this combined treatment for patients with comorbidity. The goal was to improve the symptoms of anxiety and asthma, and quality of life, and reduce the use of albuterol. The study conducted two protocols, a 14-session and an 8-session treatment, for patients with comorbid asthma and PD. The 14-session protocol had a high dropout rate, leading to its reduction to the 8-session protocol. Despite recruitment challenges, both protocols showed significant reductions in PD severity, anxiety symptoms, and asthma severity. The 8-session protocol resulted in faster improvements, although effect sizes were larger in the longer protocol. Asthma symptoms and medication use significantly decreased in both protocols, with a large effect size in the 14-session protocol. Asthma quality of life improved significantly in both protocols, with large effect sizes. Albuterol use decreased significantly in the 8-session protocol, especially during the follow-up period. The therapy had limited effects on spirometry.
CBT is a psychotherapeutic approach that teaches individuals techniques to modify negative thoughts, emotions, and behaviors. When it comes to individuals who have comorbid anxiety and asthma, medications that reduce anxiety may not be the most preferred method for patients, as they do not target the underlying cause and some medications may interact with asthma treatments. While CBT has shown promise in managing anxiety disorders, more extensive and rigorous trials are needed to specifically target individuals with comorbid anxiety disorders, such as PDs, and asthma. Ross et al. [18] examined the effectiveness of an 8-week nurse-administered group treatment program for adults with asthma and coexisting PD. The program combined CBT for PD with AE. Forty-eight women with confirmed diagnoses of asthma and PD were randomly assigned to either the treatment group (n = 25) or a wait-list control group (n = 23). Twenty-five participants completed the treatment, with 15 in the treatment group and 10 in the wait-list control group. The researchers used repeated measures analysis of variance (ANOVA) procedures to compare the groups on panic and asthma outcomes at both post-treatment and a 6 month follow-up. The results showed that the CBT-AE program had significant and enduring anti-panic and antianxiety effects. It also led to substantial, though not sustained, improvement in morning peak-flow expiratory rate and asthma-related quality of life.
A 2012 study by Parry et al. [20] examined adults with asthma and anxiety and found a reduction in self-reported asthma-specific fear at the end of treatment and 6 months in those receiving individual CBT. Therapists conducted a cognitive-behavioral formulation for each patient’s asthma-specific fear issues based on an individual analysis of situational triggers, asthma-related beliefs, cognitions, attentional focus, and physiological factors. The therapy included various elements, such as explaining the differences between asthma and anxiety symptoms, promoting awareness of anxiety-provoking cognitions, reducing somatic preoccupation, engaging in controlled exposure to anxiety, teaching methods to recognize and control hyperventilation, and exploring problematic asthma-related beliefs. This study shows how a brief cognitive-behavioral intervention can have efficacy in reducing asthma-specific panic fear immediately after treatment and at 6 months follow-up.
CBT interventions should be adapted to address the unique challenges posed by asthma triggers and fear of asthma-related situations. This could be achieved through problem-solving modules and promoting appropriate use of asthma medication and the asthma action plan [32]. A key aspect to consider is how to modify standard anxiety-reduction techniques like graded exposure, which may involve asthma triggers. Additionally, in CBT treatment for PAs, interoceptive exposure (habituation to physiological sensations associated with anxiety and panic) may require adjustment for asthma patients who experience dyspnea. Exposure therapy is widely used to treat PD by confronting patients with the distressing physical sensations associated with panic [33]. During exposure therapy sessions, patients are gradually exposed to these sensations, and as they repeatedly experience that the anticipated catastrophic outcomes do not materialize, the intensity of physiological panic symptoms decreases. The process involves restructuring the thoughts that perpetuate fear and avoidance through repeated exposures, leading to modified perceptions of these symptoms and reduced fear and avoidance [34]. However, there is a potential risk during exposure sessions. If a patient does not remain exposed to the stimuli for the duration of a PA, it could exacerbate the panic response and even lead to treatment dropout. Careful management of exposure sessions is essential to ensure positive outcomes and minimize any adverse effects on patients’ progress and treatment adherence.
Future research should focus on the development and testing of tailored CBT interventions that address comorbid anxiety and asthma. Such interventions have the potential to improve asthma quality of life and overall well-being by effectively managing anxiety symptoms in individuals with asthma.
CBT is considered the gold standard for the treatment of asthma-related anxiety, as it has achieved promising results. However, some studies have shown partial success in addressing the symptoms of PD and improving medical adherence [33, 34]. In addition, mindfulness therapy for individuals with asthma and relaxation therapy for those with increased anxiety have not shown significant additive effects with respect to control conditions [35]. Therefore it is necessary that these techniques are improved, possibly using new technological and online tools.
In a 2020 study, Bonnert et al. [36] developed an asthma-related anxiety treatment based on individual behavioral analysis. The study identified a pattern of increased reactivity to respiratory symptoms. Therefore, researchers have designed a treatment program that includes exposure exercises specifically to target and reduce the avoidance and fear of asthma-like symptoms. For example, participants were encouraged to engage in exercise to confront and expose themselves to symptoms similar to asthma, such as increased breathing.
In a 2021 feasibility study, conducted by the same research team the treatment has been standardized for online delivery to improve accessibility, especially considering that asthma-related anxiety is a condition that is often treated by psychologists [21]. The primary objective of the study was to assess the feasibility and potential effectiveness of the online CBT program. Additionally, researchers aimed to explore whether the goal of treatment, which included reducing avoidance over behaviors triggered by asthma anxiety (such as excessive checking of inhaler availability, avoidance of physical activities or environments perceived as asthma triggers, frequent monitoring of respiratory symptoms, and increased reliance on rescue medications), led to successive reductions in anxiety-related to asthma. This study involving 30 participants aged between 18 and 75 with a physician’s diagnosis of asthma, reported worry about asthma. Data was collected at multiple time points, including pretreatment, weekly during the treatment period, post-treatment, 2 months after treatment completion (primary endpoint), and 4 months after treatment completion. Various assessments were used to measure treatment credibility, perceived alliance, treatment satisfaction, adequate relief, and adverse events. The primary outcome measure was “CAS”, and secondary outcomes included asthma control, fear of asthma symptoms, asthma-related avoidance behavior, worry, anxiety sensitivity, perceived stress, and quality of life. The 8-week online treatment was therapist-guided and included weekly modules focusing on education about asthma, the role of fear and avoidance behavior, affective labeling, exposure exercises, and relapse prevention. The study employed multilevel linear mixed models to analyze the effects of time on the primary endpoint and weekly assessments. The results showed significant improvements in CAS and all secondary outcomes, with moderate to large effect sizes. Moreover, reductions in avoidance behavior during the treatment period were predictive of reductions in CAS in the following week. In conclusion, the study demonstrated the feasibility and potential efficacy of the online CBT program for anxiety-related asthma.
Respiratory ratio is a dimensional construct of the respiratory subtype of PD. It refers to the ratio of CO2 produced to oxygen consumed during respiration. Specifically, it is a calculation used to determine the respiratory quotient (RQ), which provides insights into the type of fuels (e.g., carbohydrates, fats) being metabolized for energy. In the context of basal metabolic rate calculations, understanding the respiratory ratio is crucial as it offers information about the metabolic substrate preferences of the body during resting conditions. This ratio aids in assessing the energy utilization patterns and metabolic efficiency of an individual. The respiratory subtype of PD has been associated with increased sensitivity to CO2 inhalation, a positive family history of PD, and low comorbidity with depression. Patients with PD show abnormal behavioral and physiological responses to respiratory challenge tests. Inhalation of CO2 increases partial pressure of CO2 (pCO2) and reduces the pondus hydrogenii (pH) in the blood, changes that are also observed in the brain. Some brain regions, sensitive to H+/CO2, have been involved in ventilation control and defensive behavior, including panic. The increase in CO2 and H+ in the brain could activate such structures, inducing PAs and increasing ventilation [37, 38].
In a 2013 study, 91 patients with PD were examined with a double inhalation of a 35% CO2 mixture [22]. The respiratory ratio was calculated based on the scores of respiratory symptoms recorded in a diary in the days before the CO2 challenge. The results showed that the respiratory ratio is actually related to CO2 sensitivity. This positive correlation suggests that the intensity of respiratory symptoms may be proportional to individual sensitivity to CO2. In particular, the sample of patients consisted of 62 “responders” (about 68.1%), that is patients who had a PA, and 29 “non-responders” (about 31.9%) who did not have PAs after the test. The respiratory symptoms triggered by the CO2 challenge accounted for 45.8% of the panic symptoms recorded in the diary of all patients.
The analysis showed a moderate and positive correlation between the respiratory ratio and the maximum possible increase in the Subjective Units of Disturbance Scale (SUDS) score, a quantitative evaluation method ranging from 0 (no anxiety) to 10 (maximum anxiety) [22]. In addition, positive correlation trends were observed between respiratory ratio and SUDS score after testing and family history of PD, while a negative correlation between respiratory ratio and education was observed.
Analysis of the receiver operating characteristic (ROC) curve provided an area below the curve of about 0.707 for the respiratory ratio, with a cut point in the respiratory ratio of 0.437 [22]. Using this cutting point, the respiratory ratio sensitivity in predicting CO2-induced PAs was 67.7%, with a specificity of 80.8%. Overall, these findings provide valuable insights into the significance of the respiratory ratio as a potential marker for understanding the respiratory subtype of PD. It may offer a promising avenue for linking psychopathological manifestations to the underlying neurobiology, thereby enabling more targeted and effective therapeutic interventions in the management of PD.
Another significant study related to the respiratory subtype of PD is that of Maddock et al. [39]. In this study, the investigation focused on neurometabolic abnormalities in PD, particularly exploring activity-dependent changes in brain metabolites. The research involved 21 PD patients (13 in remission, 8 symptomatic) and 12 healthy volunteers, utilizing magnetic resonance spectroscopy to measure lactate and glutamate and glutamine (Glx) combined signal from Glx responses in the visual cortex during visual stimulation. The findings revealed that PD patients exhibited significantly increased activity-dependent brain lactate accumulation compared to healthy volunteers. Notably, this elevation was consistent in both remitted and symptomatic PD patients. Conversely, activity-dependent changes in Glx were significantly diminished in PD patients, indicating a disruption in metabolic responses. Additionally, the temporal correlation between lactate and Glx changes was notably weaker in PD patients compared to control subjects. These results challenge the notion of a general upregulation of activity-dependent brain metabolic responses in PD, suggesting that heightened lactate responses may represent a trait feature of the disorder. The study proposes a model linking increased lactate levels and pH dysregulation in the brain to altered functioning of acid-sensitive fear circuits, contributing to the trait vulnerability observed in PD.
However, further research and larger-scale studies are warranted to solidify these promising observations and fully comprehend the clinical implications of the respiratory ratio in the context of PD.
The literature provides substantial evidence supporting the association between asthma and PDs [40]. Various theories have been proposed to explain this comorbidity, some of these include the dyspnea-fear theory, which attributes the link to somatic effects of hyperventilation, as well as abnormal sensitivity of CO2 receptors and “choking detectors” in the central nervous system [40]. Medications such as adrenergic agonists, theophylline, and steroids, commonly used in asthma management, have also been implicated in provoking anxiety [23, 40]. A recent prospective community study, reported in this review, showed bidirectional longitudinal associations between panic and asthma [18]. The study suggested a dose-response relationship, where active asthma predicted subsequent PD, and vice versa, even after accounting for gender, smoking, and socioeconomic status as confounders [18].
About the treatments that can be offered to patients suffering from these two disorders, it is necessary to implement a multidisciplinary, medical, and psychological approach, which allows to intervene simultaneously on the psychological and physiological state of the suffering person. A systematic review conducted by Yorke et al. [41] assessed the efficacy of psychological interventions for adults with asthma and included 14 randomized controlled trials with various psychological approaches. The reviewers highlighted several limitations, such as poor methodological quality, small sample sizes, diverse interventions, and outcome measures. Notably, only three studies [18, 42, 43] employed comprehensive CBT interventions. A meta-analysis of two of these studies [42, 43] revealed significant improvements in asthma-related quality of life and a reduction in anxiety traits or symptoms among the intervention groups. Moreover, an additional case-control trial [44] utilizing a comprehensive CBT intervention also reported a significant decrease in anxiety levels and improvements in asthma-related quality of life.
The findings of the paper included in this Cochrane review highlight the importance of tailored cognitive-behavioral interventions for individuals with comorbid anxiety and asthma [44]. Addressing the unique challenges posed by asthma triggers and fear of asthma-related situations is crucial. Moreover, novel online treatment strategies based on individual behavioral analysis have shown potential efficacy in reducing avoidance behavior triggered by asthma anxiety. The use of online CBT therapy has gained considerable attention and popularity in recent years due to its potential to overcome geographical and logistical barriers that often restrict access to traditional face-to-face therapy [44]. Online CBT offers the convenience of receiving treatment from the comfort of one’s home, eliminating the need for travel and reducing the time and cost associated with in-person sessions. This accessibility is especially crucial for individuals with comorbid anxiety and asthma, as respiratory conditions can sometimes limit their mobility or make attending in-person therapy challenging. Online CBT platforms can be particularly effective in targeting avoidance behavior triggered by asthma-related anxiety. These platforms can provide personalized interventions based on individual behavioral analysis, enabling individuals to learn coping strategies and gradually confront their fears in a controlled and supportive environment. This feature is especially relevant for individuals who may avoid certain situations due to asthma anxiety, leading to reduced quality of life and impaired functioning.
The inclusion of studies focusing on online CBT in the review signals a forward-looking approach to mental health interventions, acknowledging the potential benefits of incorporating innovative technological tools. As technology continues to advance, it is likely that online therapies will become even more sophisticated, interactive, and tailored to individual needs. However, it is essential to recognize that while online CBT offers numerous advantages, it may not be suitable for everyone. Some individuals may prefer face-to-face interactions, or certain cases may require in-person assessments or interventions. Therefore, the integration of online therapies into the existing mental health care landscape should be done thoughtfully, ensuring that individuals have access to the most appropriate and effective treatment modalities based on their unique circumstances and preferences. By including a study related to online CBT, the review sheds light on the potential of digital mental health solutions to improve the delivery of care for individuals with comorbid anxiety and asthma [44]. This work highlights the need for continuous research and development in the field of e-mental health and encourages practitioners and researchers to explore new ways of providing evidence-based interventions to a broader population, ultimately enhancing the overall quality of care for those experiencing these challenging comorbid conditions. The respiratory subtype of PD, characterized by increased sensitivity to CO2, provides valuable insights into the underlying neurobiology, suggesting potential markers for targeted therapeutic interventions [5]. It is evident that the relationship between asthma and PDs is complex and multifaceted, involving both physiological and psychological factors. Further research is warranted to better understand the underlying mechanisms and develop targeted interventions to improve the management of comorbid PD and asthma.
While conducting this systematic review on the link between PD and asthma, several limitations have emerged that need to be acknowledged. Firstly, the available literature predominantly focuses on the physiological aspects of asthma in PD, often neglecting potential psychological and social factors that could contribute to symptom development and severity. A more comprehensive analysis that incorporates these multifaceted influences could provide a more holistic understanding of the disorder and its treatment. Moreover, the heterogeneity among the studies included in this review poses a challenge. Variability in methodologies, sample sizes, and diagnostic criteria may lead to difficulties in comparing and synthesizing the results. Lastly, despite the potential implications of this review for improved health outcomes and psychological interventions for panic management, there is a need for further research in this area. Larger randomized controlled trials with standardized interventions, taxonomy, and outcome indicators are needed to better understand the efficacy of CBT interventions for individuals with both asthma and clinical anxiety. By conducting more robust studies, evidence-based guidelines can be established for tailored interventions aimed at improving the well-being and health outcomes of individuals with comorbid anxiety and asthma.
Despite these limitations, this systematic review provides a valuable foundation for future research and practice in the field of PD and respiratory disorders. By recognizing and addressing these challenges, researchers can design more robust studies and develop tailored interventions to enhance the overall well-being and quality of life of individuals experiencing PD and concomitant respiratory symptoms.
This review has meticulously explored a multitude of studies investigating the correlation between PD and asthma. The emphasis has been on studies that delve into the psychological implications for individuals grappling with both conditions. By comprehensively exploring both psychological and physiological dimensions, the way can be paved for more targeted interventions that address the distinctive challenges faced by individuals dealing with PD and asthma. Empowering clinicians and researchers to zero in on these specific vulnerabilities not only enhances the treatment and support for individuals with PD but also raises the overall standard of care. The advancement of knowledge and the promotion of a holistic approach to management hold the potential to significantly enhance the well-being and quality of life for those affected by this dual burden. Through ongoing research and collaborative efforts, a brighter future for individuals contending with PD and asthma can be envisioned, offering them the hope of attaining higher standards of quality of life.
5-HT: serotonin
AE: asthma education
CAS: catastrophizing about asthma
CBT: cognitive-behavioral therapy
CO2: carbon dioxide
GABA: gamma-aminobutyric acid
Glx: glutamate and glutamine
PAs: panic attacks
PD: panic disorder
GCP: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. The author read and approved the submitted version.
The author declares that she has no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2024.
Copyright: © The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

Amar P. Garg ... Bajeerao Patil
Jim E. Banta ... James M. Banta
Nassiba Bahra ... Samira El Fakir
Silvina Monica Alvarez ... Nidia Noemi Gomez
Alberto Vidal, Marcela Matamala