Original Article
Original Article

Affiliation:
1Dermatology Unit, Department of Internal Medicine, Faculty of Clinical Sciences, University of Abuja, Abuja PMB 117, Nigeria
Email: perpetua.ibekwe@uniabuja.edu.ng
ORCID: https://orcid.org/0000-0003-1827-1362
Affiliation:
2Department of Paediatrics, Faculty of Clinical Sciences, University of Abuja, Abuja PMB 117, Nigeria
ORCID: https://orcid.org/0000-0003-0536-8317
Affiliation:
3Department of Haematology and Blood Transfusion, Faculty of Basic Clinical Sciences, University of Abuja, Abuja PMB 117, Nigeria
ORCID: https://orcid.org/0000-0002-9452-7115
Affiliation:
4Department of Internal Medicine, Faculty of Clinical Sciences, University of Abuja, Abuja PMB 117, Nigeria
ORCID: https://orcid.org/0000-0003-4672-0700
Affiliation:
1Dermatology Unit, Department of Internal Medicine, Faculty of Clinical Sciences, University of Abuja, Abuja PMB 117, Nigeria
ORCID: https://orcid.org/0000-0002-3420-1826
Explor Asthma Allergy. 2024;2:450–460 DOI: https://doi.org/10.37349/eaa.2024.00057
Received: March 30, 2024 Accepted: May 15, 2024 Published: September 06, 2024
Academic Editor: Somasundaram Arumugam, National Institute of Pharmaceutical Education and Research, India
The article belongs to the special issue Atopic Dermatitis – Pathology and Treatment modalities
Aim: Few reports on atopic dermatitis (AD) in adults from Africa exist in the literature. AD in adults can occur as childhood-onset, in which AD begins in childhood and continues till adulthood, or adult-onset, in which AD develops in adulthood. Typical appearance of AD includes acute or chronic eczematous lesions recurring or chronic in nature that is symmetrically distributed on flexural body surfaces. Atypical clinical patterns and morphology are commonly described among the adult population. The purpose of this study is to describe the frequency, clinical pattern, and contact sensitization of adults with AD.
Methods: A prospective study of patients seen at the dermatology clinic of a tertiary referral center in Abuja, Nigeria, between September 2020 and September 2022. Adult patients who fulfilled at least three major and three minor criteria of the Hanifin and Rajka guidelines were recruited. The Patient-Oriented SCORing Atopic Dermatitis (PO-SCORAD) index for black skin was used to determine AD severity. Contact sensitivity was assessed using a modified European baseline series and skin prick testing of common aeroallergens was also done.
Results: Out of a total of 2,177 patients, only 38 adults were diagnosed with AD. Two-thirds of them had adult-onset AD. The majority (63.2%) had chronic eczema at presentation, 23.7% had perifollicular accentuations, and 13.2% had acute eczema. The mean SCORAD index was 20.5 (16.4 to 24.6). The mean eosinophil count was 5.9 ± 3.4 cells/dL. The skin prick test revealed sensitization to at least one allergen in 68.8% of the patients. Contact sensitivity to methyldibromoglutaronitrile, lanolin, and paraben was highly observed.
Conclusions: Adult-onset AD is more common than childhood-onset AD in adults. The morphology and distribution of eczema did not differ from other studies. Adult AD individuals tend to develop contact sensitivity to preservatives.
Atopic dermatitis (AD) is a chronic inflammatory skin disease that commonly affects the flexural regions of the body. It is characterised by itching and eczematous patches that can impair greatly the patient’s quality of life. It is not as common in adults as in children. Few reports on AD in adults from Africa exist in the literature [1], and there are no clinic-epidemiological studies from Nigeria. The prevalence of AD in the adult population conducted in the United States, Canada, France, Germany, Italy, Spain, United Kingdom, and Japan was reported in 2018 to vary from 0.3% to 10.7% [1], and in 2023 from the AWARE 1 study [2] conducted in Argentina, Brazil, China, Colombia, Egypt, Israel, Malaysia, Mexico, Russia, Kingdom of Saudi Arabia (KSA), Singapore, Thailand, Turkey, and United Arab Emirates to vary from 3.4% to 33.7%. Variation in prevalence depends on the population being studied, disease definitions, and methodology [1]. AD in adults can occur in two forms: childhood-onset AD, in which AD begins in childhood and continues into adulthood, and adult-onset AD, in which AD develops in adulthood. A study in Southeastern Nigeria by Nnoruka [3] reported that 24.5% of patients with AD had adult-onset AD. The characteristic clinical features of AD differ across life phases, with infantile AD presenting with erythematous papulovesicular lesions on the face and extensors and childhood AD presenting with xerosis and lichenified lesions on flexural extremities. Although similar features can be observed in adult AD, it is expected that atypical morphologies can also occur since the physical and environmental conditions affecting adults differ from those in children [4]. There are also differences in the clinical appearance and morphology of AD with different skin types. For example, follicular accentuations are commoner in the black skin.
Adults with AD may manifest various clinical features including chronic lichenified eczema, psoriasiform dermatitis, and hand dermatitis [4]. Also, the distribution of eczema in adults can become more generalised. Despite these reports, the Hanifin and Rajka criteria are still the gold standard for the diagnosis of AD in adults [5]. This criterion requires the presence of three major (any of the following: pruritus, presence of typical morphology and distribution of AD lesions, chronic or chronically relapsing dermatitis, and personal or family history of atopy) and three minor criteria to make a diagnosis of AD (see Table 1). Although the criteria have been modified for use in different countries, most of these populations maintain the typical morphology and distribution of AD (eczematous lesions in the flexural region in persons other than infantile) as a major criterion. One of the major criteria in the UK Working Party guidelines [6], that is, onset prior to 2 years of age does not recognise the possibility of adult-onset AD. While the Japanese guidelines do not include the presence of a personal or family history of atopy and exclude other minor criteria such as elevated serum IgE levels in making a definitive diagnosis of AD [7]. Although the Chinese guideline for diagnosing adult or adolescent AD is simply three items, like the Japanese criteria, it has yet to be widely adopted [8] (see Table 1).
Diagnostic criteria of atopic dermatitis by Hanifin and Rajka, UK Working Party, Japanese Dermatological Association, and Chinese guidelines for adolescent/adults
| Hanifin and Rajka criteria | UK Working Party | Japanese Dermatological Association guidelines | Chinese guidelines (adolescents/adults) |
|---|---|---|---|
Major features:
Minor features:
| Major feature:
Minor features:
Diagnosis: major plus three or more of the minor features | Major features:
Diagnosis: All above features must be present for more than 2 months in infancy and more than 6 months in childhood, adolescence, and adulthood. | Major feature:
Minor features:
Diagnosis: major plus one or more of the minor features |
One alternate diagnosis often made in adults with eczematous conditions is allergic contact dermatitis (ACD) and airborne contact dermatitis, and often patch testing is used to exclude this diagnosis [4]. AD patients have a familial tendency to develop Th2 responses against common environmental antigens [9], and this predisposes them to aero and cutaneous sensitization. Meanwhile, the relationship between AD and ACD is still debatable. It is debatable whether AD patients have an increased risk for contact sensitization when compared with controls, as the systematic review by Hamann et al. [10] on epidemiological studies of contact sensitization in AD compared with non-AD patients reported mixed results.
The prevalence of AD appears to be increasing in Nigeria, and the current prevalence from a meta-analysis of studies in Nigeria puts it at 10% [11]. Most of the studies were mainly on children, and data on adults with AD is lacking. The purpose of this study is to describe the frequency, clinical pattern, and contact sensitization of AD in adults.
This is a prospective study of adult patients with AD seen at a tertiary referral centre, between September 2020 and September 2022. Patients aged 18 years and older who fulfilled the Hanifin and Rajka diagnostic criteria for AD, were presenting for the first time, and were not on any treatment at the time of enrolment were consecutively recruited during the study period. AD was diagnosed by the dermatologists. Any patient who was on systemic steroids and who had extensive dermatitis involving their upper backs, were excluded from patch testing; any patient who was on systemic antihistamines for more than a week was excluded from skin prick testing, while known AD patients that were symptom-free at the time of the study were excluded from the study.
The criteria for the diagnosis of AD were based on the Hanifin and Rajka guidelines [5]. Patients fulfilling at least three major, and three minor criteria were considered to have AD. The major criteria included the presence of pruritus, typical morphology and distribution of eczema, a chronic relapsing course, and a personal or family history of atopy. Typical morphology includes presence of papules, vesiculopapules, exudation, scales, and crust for acute lesions and lichenification, scales, thickened skin, and infiltrated erythema for chronic lesions. Typical distribution includes symmetrical involvement of flexural surfaces of arms and legs, neck, anterior chest, and back. A family history of atopy was regarded as the presence of a first-degree relative with either one or more histories of physician-diagnosed allergic rhinitis, AD, allergic conjunctivitis, or asthma. The age of onset of AD and family history (in parents, siblings, and children) of AD, asthma, allergic rhinitis, and conjunctivitis were obtained based on the patient’s self-report. A skin prick test (SPT) was used to assess for the presence of immediate (type 1) skin reactivity and food intolerance, two of the Hanifin and Rajka minor criteria [5]. Total serum IgE, keratoconus, and anterior subcapsular cataracts were not assessed.
Acute eczema was defined by the presence of vesicles, oozing, and crusting; chronic eczema was defined by lichenification with epidermal thickening and post-inflammatory hyperpigmentation; and perifollicular accentuation was defined as dermatitis enhanced around hair follicles and has a diameter of more than 5 cm in two or more areas of the body [12]. Dennie-Morgan fold was diagnosed as a line or a crease below the lower eyelid; hyperlinearity of the palms was defined by the presence of more than 5 prominent lines longer than 1 cm running across the palms; and keratosis pilaris was diagnosed as the presence of 20 keratotic, follicular papules clustered (“chicken skin appearance”) at least in the posterolateral arms and/or thighs [12].
The Patient-Oriented SCORing Atopic Dermatitis (PO-SCORAD) index for black skin [13] was used to determine AD severity. The SCORAD consists of score for extent and intensity of the lesions, sleep loss, and pruritus. Extent of involvement was scored using the rule on nine. Intensity of the lesion was scored for redness/pigmentation, swelling/papulation, dryness, oozing/scabs, excoriation marks and skin thickening, and subjective scores were obtained for pruritus and sleep loss. The range of the SCORAD score is between 0 and 103 points. This was performed at the presentation by the physician and categorized as mild if the total score was less than 25, moderate if within 25 to 50, and severe AD if it was above 50 [13].
Demographic information was obtained from the participants, such as personal history of asthma, allergic rhinitis, allergic conjunctivitis, age of onset of lesions, morphology of eczema, presence of other minor AD criteria, and type of moisturizers being used by the patient in the past 3 months. SPTs, eosinophil counts, and patch testing were done for each participant. Two millilitres of whole blood collected into EDTA vacutainer tubes from patients was analysed within one hour at the Haematology Department of the University of Abuja Teaching Hospital, Gwagwalada. Evaluation of eosinophil count and percentage were performed by flow cytometry measurement in the full blood count and differential count of white blood cells using the Mythic-22 OT (Orphee Switzerland) automated haematology analyser following the manufacturer’s operational guidelines. Five cells/dL or more of the eosinophil count were considered high, and less than that was considered normal.
SPT against aspergillus niger, candida albicans, cockroaches, dog dander, blomia tropicalis, dermatophagoides pteronyssinus, dermatophagoides farinae, chenopodium album, cow milk, cereal mix, bermuda, peanut, cod fish, and whole egg allergens from ImmunoTek (Spain) were done. It has a high specificity and a high positive predictive value in determining serum specific IgE [14]. SPT was done after the first consultation. Sterile saline and histamine (10 mg/mL) were used as negative and positive controls, respectively. It was performed on the inner forehand of the patient, as previously described [15]. A drop of the different allergens was placed 2 cm apart, and a lancet with a 1 mm tip was used to prick the skin over the droplet. Reading was taken 15 minutes after the prick. A positive reaction was regarded as a wheal ≥ 3 mm in diameter and compared with the positive and negative controls.
Patch testing was as previously described [16]. Briefly, it was done using a modified European Baseline series of 28 allergens (allergEAZE®, SmartPractice, Canada) using 8 mm Finn Chambers® on Scanpor tape (allergEAZE®, SmartPractice, Canada). Benzocaine, mercapto mix, N-isopropyl-N-phenyl-4-phenylenediamine, epoxy resin, sesquiterpene lactone mix, and budesonide were replaced with carba mix, chlorhexidine digluconate, and corticosteroid mix. The allergens were placed on participants backs and read on days (D) 2 and D4. International Contact Dermatitis Research Group guidelines grade 2+ (erythema and papules) or higher was considered a positive reaction. Only readings evaluated on D4 were analysed for this study. No delayed reactions beyond D4 were monitored. In cases of positive patch-test reactions, previous and current exposures were systematically assessed for clinical relevance, and recommendations for avoidance were presented to the participants.
The data were analysed using the SPSS software, version 23. A chi-square or Fisher’s test was used for categorical variables. Statistically significant values were considered at p < 0.05.
During the study period, a total of 2,177 patients attended the dermatology clinic, of whom 38 adults were diagnosed with AD, giving a prevalence of 1.7% of patients attending the dermatology clinic. The sex ratio was approximately equal: 20 females and 18 males. The age range of study participants was 18 to 63 years, and the average age was 34.5 (95% CI 30.6–38.3) years. Most of our study participants (76.3%) were younger than 40 years of age, and the lowest population (5.3%) were older than 50 years of age.
Slightly below (18/38) 50% of the participants reside in Gwagwalada area council, which is where the dermatology clinic is located and a relatively rural (sub-urban) environment, (13/38) 34.2% reside in Abuja Municipal Area Council (AMAC), which is the largest area council in Abuja, an urban environment and about 80
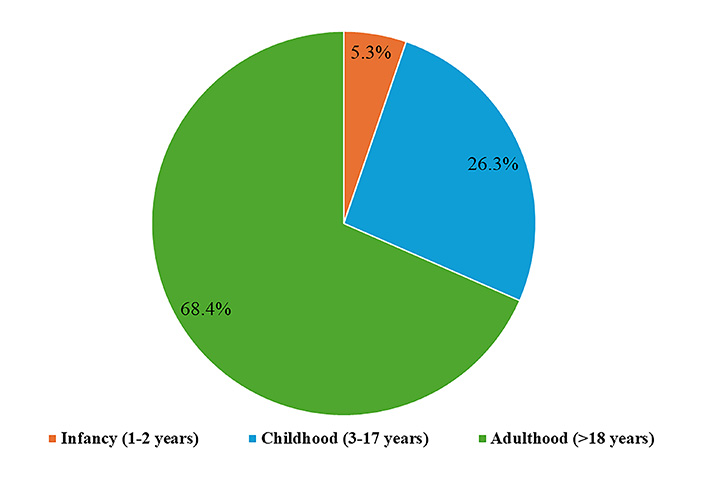
Only 2 (5.3%) of the patients have had AD since infancy; 10 (26.3%) developed AD in childhood, while two-thirds (68.4%) developed symptoms in adulthood (Figure 1). The 63-year-old patient in this study developed AD symptoms at the age of 51. The mean age (95% CI) of onset of symptoms was 22.1 (18 to 26.2) years. Most of the participants, 19 (50%), identified sweating as an aggravating factor to their symptoms; 15 (39.5%) were unaware of possible triggers; and 4 (10.5%) thought that their bathing soaps and washing detergent might be aggravating factors. Only 6 (15.8%) had a first-degree family member with AD. A family history of atopy was observed in 17 (44.7%) patients, a personal history of allergic rhinitis was present in 7 patients, a personal history of bronchial asthma was present in 2 patients, and 13 patients had a personal history of allergic conjunctivitis. Only nine (23.7%) suspected an allergen to be the cause of the recurrent lesions. The allergens suspected included perfumes, cold, dust, washing detergents, leather, fish, and water.
Most of our study participants, 24 (63.2%), had chronic eczema at presentation, 5 (13.2%) had acute eczema, and 9 (23.7%) had perifollicular accentuations. In our study, the involvement of the neck, antecubital fossae, popliteal fossa, anterior trunk, posterior trunk, and palmoplantar was noted in 27%, 43.2%, 35%, 18.9%, 18.9%, and 8%, respectively. Concomitant involvement of the forearms, arms, and thighs was observed in 45.9% of the cases.
Table 2 shows the minor criteria found in all our study participants and their frequency of occurrence. The four most common minor criteria were xerosis, Dennie-Morgan fold, immediate skin test reactivity, and hyperlinearity of the palms.
Hanifin and Rajka criteria observed in our study
| Minor criteria | Frequency (%)n = 38 |
|---|---|
| Dennie-Morgan folds | 44.7 |
| Xerosis | 52.6 |
| Hyperlinearity of the palms | 26.3 |
| Long nail ridging | 18.4 |
| Immediate (type 1) skin test reactivity–positive SPT | 57.9 |
| Anterior neck fold | 7.9 |
| Low hairline | 7.9 |
| Keratosis pilaris | 15.8 |
| Orbital darkening | 5.3 |
| Hertoghe sign | 5.3 |
| White dermographism | 5.3 |
SPT: skin prick test
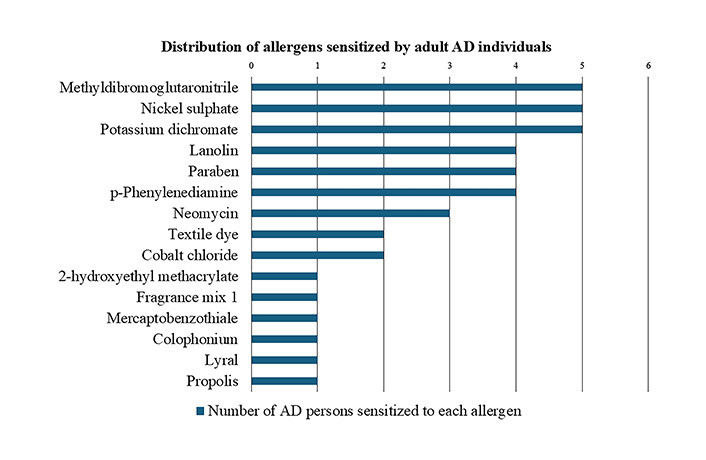
The mean SCORAD index of patients in our study was 20.5 (16.4 to 24.6). Participants had only mild (39.5%) and moderate (60.5%) AD, according to the SCORAD severity grading. The mean eosinophil count (cells/dL) observed in 68% of our patients was 5.9 ± 3.4. Almost two-thirds (16/26) 61.5% of them had an eosinophil count of 5 cells/dL or above. A SPT done in 32 patients (84.2%) revealed sensitization to at least one allergen in 68.8% of the patients. Most of them (12/22), were house dust mites (54.5%) and in 7 of 22 patients were cockroach epithelia (31.8%). The percentage of patients with sensitization to grass pollen was (4/22) 18.2%, fungi was (2/22) 9.1%, and food was the least, with 4.5%. Regarding contact sensitivity from patch testing, about 57.9% (22/38) of our AD patients were sensitized to at least one allergen. The five top allergens are methyldibromoglutaronitrile (MBGN), nickel sulphate, potassium dichromate, lanolin, and paraben (Figure 2); 15.8% (6/38) of AD patients had contact sensitivity to MBGN, lanolin, and paraben, while 7.9% (3/38) were to nickel sulphate and cobalt chloride. Clinical relevance could only be established in 16 (42.1%) patients (Table 3).
Clinically relevant allergens and their source
| Allergen | Source |
|---|---|
| Neomycin | Triple action creams with neomycin |
| Phenylalanine | Hair dye |
| Paraben | Paraben containing emollient |
| Methyldibromoglutaronitrile | Emollient |
| Textile dyes | Dark coloured clothing |
| Methyldibromoglutaronitrile | Washing agents |
| Cobalt dichloride | Leather shoes |
| Fragrance mix 1 | Cosmetics |
| Colophonium | Cosmetics |
| Phenylalanine | Occupational dermatitis |
| Propolis | Cosmetics |
| Mercaptobenzothiazole | Rubber products |
| Nickel sulphate | Jewellery |
| Nickel sulphate | Jewellery |
| Paraben | Emollient |
| Lanolin | Emollient |
All the patients were treated with mild to moderately potent topical corticosteroids (1% hydrocortisone, methylprednisolone, and betamethasone valerate 0.1%) and moisturizers (urea cream, Aveeno®, and Sebamed Body Milk®). Systemic antibiotics (erythromycin) and short courses of systemic steroids were prescribed for patients with moderate AD. There was no statistically significant difference between a positive family history of atopy (p = 0.6), allergen sensitization (p = 0.08), eosinophil count (cells/dL) (p = 0.7), and SCORAD (p = 0.6) between those with persistent AD and adult-onset AD.
This study provides a clinical and epidemiological profile of adults diagnosed with AD at a tertiary hospital located in Nigeria. The period prevalence observed in our study among adults with AD attending the dermatology clinic was 1.7%. This finding is lower than that reported among children with AD in another Nigerian study [7]. This is expected, as AD is globally known as a childhood disease. However, our study prevalence is higher than a similar study in another African country, Madagascar (0.5%) [17], almost close to that reported in Cameroun (2.1%) [18] but far lower than those reported recently by an international survey done in Argentina, Brazil, China, Colombia, Egypt, Israel, Malaysia, Mexico, Russia, KSA, Singapore, Thailand, Turkey, and the United Arab Emirates [2]. This international survey was a web-based cross-sectional study and used UK working criteria, while the study from Madagascar, just like ours, was hospital-based and used Hanifin and Rajka criteria. There is also the possibility of differences in climatic and socioeconomic conditions. The fact that we were able to diagnose adult patients with AD emphasizes the fact that AD is not just a childhood disease but can persist and develop in adults.
Most of our patients were younger than 40 years of age, and the least common age group with active AD was older than 50 years of age. This is similar to an adult AD study in Finland, where the prevalence of AD was observed to decrease with age [19] but contradicts a UK study where the prevalence of adult AD increased with age [20].
Our study observed a higher percentage of individuals (68.4%) who developed AD after the age of 18 years, this is higher than that reported almost 20 years ago in a study from Southeastern Nigeria where 15.5% developed AD after the age of 18 years [3]. A similar trend was observed by Kiiski et al. [19]. Apparently, not only is the prevalence of AD globally on the rise, but the number of people who develop AD in adulthood (adult-onset AD) is also on the rise.
In our study, adult-onset AD was not associated with an increased frequency of allergic rhinitis, bronchial asthma, or allergic conjunctivitis. This is in keeping with the results of a systematic review and meta-analysis of the prevalence and phenotype of adult-onset AD reported by Lee et al. [21]. A little less than 90% of our patients were sensitized to at least one allergen with a SPT, with sensitization to house dust mites being more frequent. Visitsunthorn et al. [22] have shown that SPT has significantly comparable sensitivity, specificity, positive predictive value, and negative predictive value with specific IgE levels. Our report in which house dust mites’ sensitization was the most frequent is similar to a study by Dey et al. [23]. There are conflicting reports on the relationship between house dust mites and AD. Some studies have documented a direct relationship between indoor house dust mites’ levels and AD symptoms [24, 25] while others have reported no significant association between house dust mites’ exposure and AD severity [26, 27]. Kim et al. [28] reported that an exposure to house dust mites increases the severity of symptoms in AD patients, especially in patients without sensitization to house dust mites and their findings suggest house dust mites can act both as an irritant as well as an allergen.
Clinical characteristics of adult AD in Nigeria have not yet been described, and very little literature from other African countries exists. We observed that although most of our patients had eczema on the flexural elbows, popliteal fossa, and neck, involvement of the trunk, forearms, and thighs was frequently observed. Similar distributions of typical AD morphology and involvement of flexural and non-flexural areas have been reported in other studies [8, 17, 29, 30]. This shows that Hanifin and Rajka criteria can be used to diagnose adult AD. Like the study from Madagascar [17], most of our patients had moderate disease. However, the severity of adult AD tends to vary across studies and on the measuring instrument [2].
Slightly more than half of our patients had contact sensitivity to at least one allergen. When compared with a similar work [31], there was no significant difference observed. Due to the impaired cutaneous barrier and immune dysregulation of AD patients, there is a need for frequent use of emollients and topical medications leading to an increase in the penetration of allergens which then predisposes AD patients to develop ACD. A systematic review and meta-analysis of association between AD and contact sensitization showed that contact sensitization to common allergens is higher in AD compared to non-AD individuals, especially in the general population, and recommended patch testing for AD patients when ACD is suspected. The allergens AD individuals are sensitized to vary across studies. However, some large patient cohort studies have shown higher rates of contact sensitization to preservatives among the AD population [32, 33]. AD patients are more likely to have contact sensitivity to preservatives found in cosmetic or dermatological products commonly used in their care and treatment.
Our study limitations include being a single study centre, which may not be generalized to the populations of other cities in Nigeria. Also, since the study population was recruited from a tertiary hospital, selection bias is inevitable, as most patients visiting a tertiary hospital have better financial status and are more likely to have medical insurance than the average patient. This could also account for the low prevalence of AD reported in this study.
In conclusion, this study provided an informative profile of AD in adult patients presenting to a tertiary dermatology clinic in Abuja. The prevalence of adult AD is lower than that reported in developed countries. Adult-onset AD is more common than persistent AD, and patients commonly have moderately severe disease. The morphology and distribution of eczema did not differ from those reported in adult AD in other studies. Adult AD patients tend to develop contact sensitivity to preservatives commonly used in cosmetic or dermatological products. More studies from other centres across the country and population-based studies are required to confirm the unique clinic-epidemiological characteristics of adult AD among skin of colour individuals.
ACD: allergic contact dermatitis
AD: atopic dermatitis
D: day
PO-SCORAD: Patient-Oriented SCORing Atopic Dermatitis
SPT: skin prick tests
We wish to acknowledge the financial support received from the Institution-based Research grant of the Nigerian Tertiary Education Trust Fund, the nursing and record staff of the dermatology clinic, and the patients who gave consent to participate in this study.
PUI: Conceptualization, Investigation, Writing—original draft, Writing—review & editing, Funding acquisition. EE: Conceptualization, Investigation, Writing—original draft. TO: Investigation, Writing—review & editing. PB and BAU: Validation, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
The atopic dermatitis in adults: prevalence, clinical pattern and contact sensitization study protocol was reviewed and approved by the University of Abuja Teaching Hospital Health Research Ethics Committee, approval number: UATH/HREC/PR/2020/016/008 and was conducted in full conformance with the principles of the “Declaration of Helsinki”, Good Clinical Practice (GCP), and the laws and regulations of Nigeria.
A signed, written informed consent was obtained from each study participant.
Not applicable.
The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservations, to any qualified researcher.
This work was conducted with funding received from the Institution-based Research grant of the Nigerian Tertiary Education Trust Fund. The fund was used in the collection of the data. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2024.
Copyright: © The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

Gael Tchokomeni Siwe ... Stefan Barth
Serap Maden
Luis Angel Hernández-Zárate ... Víctor González-Uribe
Antara Baidya, Ulaganathan Mabalirajan
Amrita Sahu ... Somasundaram Arumugam