Review
Review

Affiliation:
Unit of Pediatric Pulmonology, Clínica MEDS, Santiago 7690000, Chile
Email: alberto.vidal@meds.cl
ORCID: https://orcid.org/0000-0002-8819-9127
Explor Asthma Allergy. 2025;3:100965 DOI: https://doi.org/10.37349/eaa.2025.100965
Received: November 07, 2024 Accepted: December 06, 2024 Published: January 10, 2025
Academic Editor: Nelson A. Rosario Filho, Federal University of Parana, Brazil
Severe pediatric asthma is a very challenging type of asthma for both physicians and patients. Precision medicine in severe pediatric asthma has undergone important developments in recent years. This therapeutic approach requires an adequate diagnosis and clinical phenotyping of patients and is useful for predicting the prognosis and response to treatment in this type of patient. This article summarizes the scientific information of the last five years in the diagnosis of severe pediatric asthma, focusing on topics such as genetic markers, biomarkers, lung function, radiological techniques, and bronchoscopy.
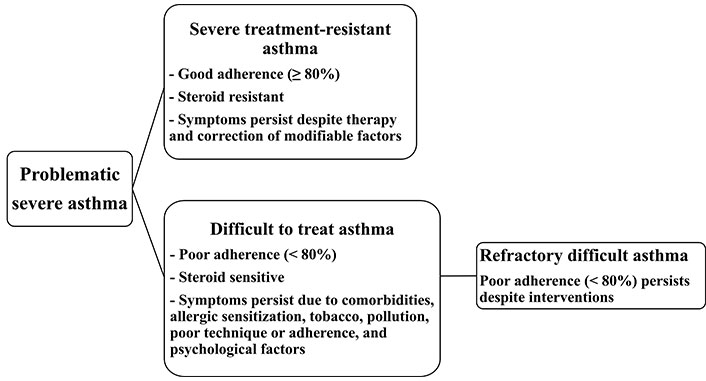
Asthma is a common condition in children and adolescents. Recently, the Global Asthma Network (GAN) reported an asthma prevalence of 12.8% for children and adolescents [1]. Although most children and adolescents have mild-moderate asthma, there is a group of severe asthmatics whose evolution is associated with greater morbidity, mortality, health costs, and persistence of the disease into adulthood [2, 3]. A recent meta-analysis conducted in Europe reported a prevalence of severe asthma in children and adolescents of 3% with no significant differences by gender [4]. In 2014, American Thoracic Society/European Respiratory Society (ATS/ERS) consensus was published, defining severe asthma for children, adolescents, and adults. ATS/ERS consider severe asthma as a condition requiring high doses of inhaled corticosteroids (ICS), plus a second controller drug or use of systemic corticosteroids [5]. The latest update of the Global Initiative for Asthma (GINA) proposes a retrospective classification to define the severity of asthma, which considers the treatment necessary to control symptoms and exacerbations for at least two or three months, allowing the identification of patients with asthma refractory to treatment with high doses of ICS plus long-acting bronchodilators, and who could benefit from biological therapy [6]. The term problematic severe asthma has gained acceptance in recent years, as it allows for a personalized clinical approach. Problematic severe asthma remains symptomatic despite maximum therapy and can be divided into severe treatment-resistant asthma (STRA), difficult asthma (DA), and refractory DA (RDA) [7]. DA can have multiple causes that can coexist, including poor adherence to treatment and/or poor inhalation technique, the presence of untreated comorbidities, exposure to allergens or environmental pollutants, and even psychological stress [8]. When all modifiable factors in DA have been identified and controlled and the patients remain symptomatic nonetheless, we are in the presence of STRA, which is a type of asthma resistant to corticosteroids due to variable mechanisms and which requires further study [9]. Figure 1 shows the categories of problematic severe asthma.
The rapid advancements of precision medicine in pediatric asthma have allowed us to identify phenotypes, endotypes, genetic markers, and biomarkers that have helped us better understand the mechanisms of severe asthma [10]. This has also allowed the advancement of personalized therapy in severe pediatric asthma and the increasingly safe and effective incorporation of biological drugs [11]. This article aims to analyze the evidence in the diagnosis of severe asthma in children and adolescents in recent years.
A review of the scientific evidence on severe pediatric asthma between October and November 2024 was conducted. Studies from the last five years were collected from different scientific databases (Medline, Web of Science, EBSCO Host, Science Direct, and SCOPUS databases). Two categories were used for the search: i) pediatric or childhood and ii) severe or difficult-to-treat asthma. The articles found were divided into five groups: genetic markers, biomarkers, lung function, radiological techniques, and bronchoscopy (BC).
The study of the human genome has allowed the discovery of new genes involved in pathogenesis, interaction with the environment, and response to treatment in pediatric severe asthma [12]. Genome-wide association studies (GWAS) performed in children and adolescents with asthma of different ethnicities have demonstrated the association between single nucleotide polymorphisms (SNPs) or novel genetic loci with severe asthma exacerbations [13–15] and severe early-onset asthma [16, 17]. An investigation conducted in children and adolescents with asthma demonstrated that PRKG1 gene expression is related to variability in response to short-acting β2-adrenergic receptor agonists (SABAs) in certain populations such as African Americans or Latinos/Hispanics [18]. Another similar study found that the expression of the DNAH5 gene (related to the movement of respiratory cilia) is associated with the variability of the bronchodilator response (BDR) in Puerto Rican children and adolescents [19]. The relationship between genetics and the response to ICS has also been the subject of study in recent years. New age-dependent genetic polymorphisms associated with the response to ICS have been identified in adult and pediatric asthmatic patients, such as THSD4, HIVEP2, DPP10, and HDAC9, which would be related to asthma susceptibility, severity, and exacerbations [20]. In the peripheral blood mononuclear cells (PBMCs) of children and adolescents with difficult-to-control asthma, decreased expression of the alpha corticosteroid receptor and a lower in vitro corticosteroid response have been found than in easily controlled asthmatics [21]. The microRNAs (miRNAs) are small RNAs (20–24 nucleotides) involved in the pathogenesis of some chronic pediatric diseases such as asthma [22]. Intercellular communication of miRNAs is carried out through exosomes, which are small extracellular vesicles that allow miRNAs to participate in the processes of inflammation, hyperreactivity, and airway remodeling in asthma [23]. The CACNA2D3 and WNT5A intergenic region has been associated with exacerbations in children and young adults, despite a history of treatment with ICS [24]. It has also been shown that blood miRNAs in children and adolescents with asthma are associated with a poorer response to treatment with ICS [25]. Another study in children and adults created a polygenic machine learning predictive model for corticosteroid response, which could provide more information for clinical decision-making [26]. A miRNA sequencing study in children and adolescents with asthma identified two circulating miRNAs (miR-1246 and miR-200b-3p) that were associated with the prediction of BDR and that were also replicated in cohorts of adult asthmatics, which would help to establish differences in response to treatment [27]. Elevated levels of two miRNAs (miR‐378a‐3p and miR‐144‐3p) have also been found in children and adolescents in patients with increased use of rescue bronchodilators, a condition that is associated with uncontrolled asthma with more symptoms [28]. In another study, five miRNAs (miR-532-3p, 296-5p, 766-3p, 7-5p, and 451b) were found to be associated with severe exacerbations of pediatric asthma and severe exacerbations in chronic obstructive pulmonary disease (COPD) in adults, possibly indicating that there are common genomic mechanisms between both conditions [29]. A study with miRNAs such as miR-210-3p has been negatively associated with regulatory T cells (Tregs), which are cells that participate in maintaining the balance of the allergic response. In addition, miR-210-3p proved to be a genetic marker that could be used to predict the severity of pediatric asthma [30]. In children with severe asthma, gene regulatory enhancers in leukocytes have been identified as different from those in mild asthmatics [31]. Epigenome-wide association study (EWAS) in asthma allows medics to analyze the interaction between genetics, environment, and response to treatment. Recently the DNA methylation (DNAm) in blood cells, nasal and bronchial epithelium has been related to the variability of the BDR in children and adolescents with moderate to severe asthma [32–34]. A study that analyzed the rs4986791 polymorphism of the toll-like receptors (TLRs) showed that pediatric patients with moderate asthma and heterozygous genotype more commonly developed severe asthma than patients with homozygous genotype [35]. In adolescents with severe asthma, the interleukin-10 (IL-10) polymorphisms rs3024498 were associated with poor control and IL-17 polymorphism rs3819024 genes with lower BDR [36]. Finally, the +2044G>A polymorphism of IL-13 gene was associated with the severity of pediatric asthma [37].
With the advancement of precision medicine, the use of biomarkers is attaining increasing importance in the identification of endotypes (type 2 and non-type 2), prediction, and monitoring of response to new treatments (e.g., biological) in severe pediatric asthma [38, 39].
Eosinophils (EOs) are a type of granulocyte involved in the pathogenesis of asthma, whose role is not yet clearly elucidated, since they commonly increase in allergic asthma but may also be present in non-allergic asthma [40]. EOs can be measured in blood, sputum, or bronchoalveolar lavage (BAL) and in asthma have been used as biomarkers in diagnosis, prognosis, and response to treatment [41]. Blood EOs count is useful for identifying patients with severe eosinophilic pediatric asthma (≥ 150 cells/μL) who could be treated with mepolizumab (anti-IL-5), dupilumab (anti-IL-4Ra) (both approved for patients over 6 years of age), or benralizumab (anti-IL-5Ra) for patients over 12 years of age [42]. A recent study involving adolescents with severe asthma treated with mepolizumab (anti-IL-5) identified a subgroup with elevated levels of EOs subpopulations (CD62Lint and CD62Lhi) that persist with exacerbations despite receiving this biological therapy, indicating that sputum EOs may be another useful biomarker in the response to treatment in severe asthma [43].
In children and adolescents with severe uncontrolled asthma, the use of fractional exhaled nitric oxide (FeNO) with values less than or greater than 20 parts per billion (ppb) is recommended in conjunction with blood EOs levels to determine, based on age (6 to 11 years or ≥ 12 years), the most appropriate biological drug [44]. FeNO has been shown to correlate well with asthma control measured by clinical questionnaires [Asthma Control Test (ACT) and GINA questionnaire (GINAq)] in severe pediatric asthma. Children with low FeNO levels only 87% (with ACT) and 91% (with GINAq) were likely to have uncontrolled asthma [45]. Additionally, in this same investigation, it was found that the best cutoff point (Youden cutoff) to detect severe uncontrolled asthma with both questionnaires was found with FeNO levels greater than 39 ppb [45]. Finally, children with moderate-severe asthma, blood levels of EOs and FeNO have been shown to be good biomarkers to identify patients who will have severe exacerbations and predict the response to biological treatments such as dupilumab [46].
A complex network of interactions between cytokines, chemokines, and inflammatory cells has been documented in severe pediatric asthma [47, 48]. In children and adolescents with STRA, the innate lymphoid cells (ILCs) and T helper (Th) cells in blood and sputum were found at significantly higher levels than in patients with DA or recurrent respiratory infections without asthma. Additionally, the STRA group was treated with intramuscular triamcinolone and after 1 month there was a significant decrease in ILC and Th2 as well as a decrease in exacerbations and improvement in asthma control [49]. Asthma severity has also been associated with deficiencies in antioxidant mechanisms. A study in children and adolescents showed that severe asthma had significantly lower levels of serum nuclear factor erythroid 2-related factor 2 (NRF2) than mild-moderate asthma, so having a low level of NRF2 could be considered a predictor of severe pediatric asthma [50]. A retrospective study showed that severe asthmatics with recurrent symptoms had significantly higher blood levels of TLR4 and soluble intercellular adhesion molecule-1 (sICAM-1) than non-recurrent asthmatics. Furthermore, the prediction accuracy was higher when combining these two biomarkers than each one separately [area under the curve (AUC) TLR4 = 0.739, sICAM-1 = 0.726, and joint detection = 0.83, respectively] [51]. Neutrophil gelatinase-associated lipocalin (NGAL) is a molecule with antibacterial potency (siderophage sequestrant) and also a marker of acute kidney disease, which could also be related to severe asthma [52]. A study performed in asthmatic children of different severity demonstrated that NGAL levels were significantly increased in severe asthmatics compared to intermittent asthmatics and healthy controls. Receiver operator characteristic (ROC) curve analysis showed a good capacity (AUC = 0.88, sensitivity = 82%, and specificity = 76%) to predict severe asthma [53]. Myeloperoxidase (MPO) and NGAL are both molecules stored in neutrophil granulocytes and secreted after cellular activation, having significantly higher sputum levels in moderate-severe asthmatics than in intermittent asthmatics, and a good correlation with the pulmonary function of these patients [54]. Moreover, the interaction between obesity and severe pediatric asthma at the systemic inflammatory level should be mentioned, a concept currently called “meta-inflammation”, resulting in increased cytokines (IL-1β, IL-6, IL-17, IFN-γ, and TNF-α) and adipokines (cysteinyl leukotrienes, adiponectin, leptin, and resistin) [55].
The usefulness of lung function in severe asthma monitoring is fundamental. In an observational cohort of children and adolescents with asthma, it was shown that males with recurrent exacerbations have a high risk of a lower forced expiratory volume in 1 second (FEV1) across childhood [56]. A study conducted in children and adolescents compared lung function in severe and non-severe asthmatics and found that the maximum response to bronchodilators found more frequently in severe asthma was associated with more asthma exacerbations, hospitalizations, worse control, and decreased lung function at one year of follow-up [57]. A retrospective study comparing children with severe asthma, non-severe asthma, and healthy children showed that the FEV1/forced vital capacity (FVC) ratio was significantly decreased and the lung clearance index (LCI) significantly higher in severe asthmatics at the start of treatment, after a year of treatment, most severe asthmatics had significantly improved spirometric abnormalities, but the LCI remained elevated, reflecting the inhomogeneity of ventilation in this group of patients [58]. LCI was found elevated in 20% of children with severe asthma and was negatively correlated with FEV1 z-score. Severe asthmatics had significantly higher mean LCI than mild-moderate asthmatics and healthy controls [59]. Furthermore, it has been identified that within children with problematic severe asthma, the LCI of those with STRA is significantly higher than those with DA or healthy controls, which could suggest that the LCI could be a marker of STRA and the 65% of children with STRA registered a decrease in LCI after treatment with parenteral triamcinolone, which was only consistent with FeNO, but not with traditional spirometry parameters [60]. Table 1 summarizes the clinical utility of genetic markers, biomarkers, and lung function in severe pediatric asthma.
Utility of genetic markers, biomarkers, and lung function in severe pediatric asthma
| Diagnostic method | Comments |
|---|---|
| Genetic markers | They help predict the response to β2 agonists and response to inhaled corticosteroids. They can also predict asthma that will follow a more severe course and with persistence of exacerbations after treatment. |
| Biomarkers | Blood and sputum eosinophils, FeNO may precede severe asthma, exacerbations, and response to biologics. Cytokines, chemokines present in blood, inflammatory cells, or sputum are associated with severe asthma. |
| Lung function | FEV1, FEV1/FVC, and BDR identify severe asthma with higher morbidity. LCI identifies asthma with inhomogeneity, which is associated with worse lung function and severe treatment-resistant asthma. |
FeNO: fractional exhaled nitric oxide; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; BDR: bronchodilator response; LCI: lung clearance index
Recent advances in chest computed tomography (CT) have opened the door to a better understanding of obstructive disease in severe pediatric asthma. The introduction of low-dose CT allows us to objectively determine early airway remodeling in severe asthma in a safe and reliable manner [61]. In severely asthmatic children and adolescents, bronchial wall thickening (BWT) was found in 80%, air trapping (AT) in 60%, and bronchiectasis (BE) in 27%. The extent of BE correlated with greater clinical severity of asthma and no alternative diagnoses to asthma were found [62]. A study performed multi-detector CT (MDCT) on children and adolescents with severe asthma and a control group, finding that severe asthmatics had higher averages of AT index (AT%), higher percentage of airway wall thickness (AWT%), and lower mean lung density (MLD) than controls. AT% presented very strong negative correlations with FVC and FEV1 and a moderate correlation with forced expiratory flow (FEF) 25–75% [63]. A recent study comparing severe asthmatics with healthy controls in pediatric age demonstrated that both bronchial thickening (BT) and AWT% provide important information about airway remodeling, but AWT% is more specific in identifying airway narrowing relative to total airway size. In this study, it was established that AWT% ≥ 38.6% (AUC = 0.99, sensitivity = 90%, specificity = 90%) allows detecting with a high degree of certainty the early remodeling of severe pediatric asthma [64]. In children and adolescents with severe asthma, an automatic inspiratory and expiratory CT software was evaluated for the diagnosis of structural alterations [65]. In this study each bronchial generation, the bronchus-artery (BA) relationship was considered, and the outer bronchial wall diameter (Bout), artery diameter (A), BWT, and low attenuation regions (LAR) were measured. BE was defined as Bout/A ≥ 1.1, BWT as BWT/A ≥ 0.14. Using the automated method, it was found that CT with percentage of BA pairs defined as BE was 24.62% and BWT was 41.7%. Patients with LAR on CT and patients with small airway dysfunction (SAD) on spirometry (FEF 75% and FEF 25–75% z-score < –1.64) had greater BWT than those without these conditions, indicating that peripheral airway involvement in severe asthma is associated with greater structural alterations [65]. An aerosol therapy evaluation study measured ICS plus long-acting bronchodilator deposition in severe asthmatics with or without spirometry-defined SAD (FEF 25–75% and FEF 75% z-score < –1.645 and FVC z-score > –1.645) and functional respiratory imaging (FRI) is a validated technique using 3D reconstructed CT was used to measure airway aerosol deposition. Patients with SAD were shown to have increased central airway deposition and decreased small airway deposition than patients without SAD [66].
In recent years, the development of pulmonary magnetic resonance imaging (MRI) techniques has increased. A study with 129Xenon (129Xe) MRI demonstrated that children and adolescents with asthma with regional ventilation abnormalities such as ventilation defect percentage (VDP) and number of defects/slices can more accurately predict those who develop severe asthma and have greater use of health systems [67]. Another study with 129Xe MRI found that the VDP and coefficient of variation (CoV) were significantly higher in severe asthmatics before bronchodilator administration than in healthy controls. After bronchodilation, the 129Xe MRI VDP and CoV decreased significantly, in contrast to the spirometry values, which did not show any changes. The authors attributed these findings to the fact that spirometry only reflects global changes in lung function, whereas 129Xe MRI is able to more sensitively detect changes in regional ventilation inhomogeneity [68].
In recent years, the use of BC in severe pediatric asthma has had a resurgence, mainly to rule out alternative diagnoses, search for germs associated with the persistence of symptoms, or in situ measurement of inflammatory markers in patients undergoing treatment with high doses of steroids, or to identify candidates for the use of biologics [69]. In some centers where BC is routinely performed in severe pediatric asthma for diagnostic and therapeutic purposes, it has been found that persistent bacterial bronchitis, trachea or bronchomalacia, and anatomical abnormalities are the most frequently found findings [70]. When BAL is added to BC, the diagnostic yield of bacterial diseases increases, but it should be used with caution in patients with known tracheobronchomalacia or very symptomatic asthma, conditions in which worse tolerance to BAL has been reported [71]. A study in children and adolescents with severe asthma found 4 granulocytic patterns on BC with BAL: 52% paucigranulocytic, 22% mixed granulocytic, 15.9% isolated neutrophilic, and 9.5% isolated eosinophilic [72]. Patients with a mixed granulocytic or isolated eosinophilic pattern had greater clinical morbidity with greater use of systemic corticosteroids, whereas those with a paucigranulocytic or isolated neutrophilic pattern had less airflow limitation and less blood eosinophilia. Furthermore, patients with an isolated neutrophilic pattern had a greater number of bacterial pathogens isolated [72]. This last finding could be related to another investigation that BAL carried out in children and adolescents with severe asthma, finding that the predominantly neutrophilic group had proinflammatory neutrophils with greater survival and dysfunctional macrophages that contribute to perpetuating airway inflammation, deterioration of innate immunity, and susceptibility to infections [73]. BC with BAL has also helped to better understand bronchial inflammation at the molecular level. A study conducted in schoolchildren with severe asthma who used high doses of inhaled and often systemic corticosteroids showed that predominantly neutrophilic BAL is associated with a greater expression of a mixed pattern of cytokines and chemokines (Th1/Th2/Th17) in contrast to paucigranulocytic BAL, which was associated with a reduced expression of these cytokines/chemokines [74]. In schoolchildren and adolescents with severe asthma who underwent endobronchial biopsy, it was shown that both submucosal eosinophilic and neutrophilic infiltrations were associated with decreased lung function in spirometry [75]. EOs infiltration was associated with better BDR and neutrophilic infiltration was related to fixed obstruction. However, the presence of intraepithelial neutrophils was associated with better lung function, while bronchial CD8 + T cells were related to better asthma control and lower cytokine expression in sputum [75]. Ultimately, a study using BC with BAL in children and adolescents with asthma of varying severity found higher levels of thymic stromal lymphopoietin (TSLP) in severe asthma than in mild to moderate asthmatics. In the same study, the high TSLP group was found to have higher concentrations of cytokines (IL-5 and IL-1β), and lower average of the FEV1/FVC ratio than the low TSLP group [76]. Table 2 summarizes the clinical utility of CT, MRI, and BC in severe pediatric asthma.
Utility of computed tomography, MRI, and bronchoscopy in severe pediatric asthma
| Diagnostic method | Comments |
|---|---|
| Computed tomography | It can identify structural alterations in severe asthma (air trapping, bronchial thickening, or bronchiectasis) early on. It can also detect airway remodeling and small airway dysfunction and monitor the site of pulmonary aerosol deposition. |
| MRI | Functional MRI with hyperpolarized gases allows measurement of regional pulmonary ventilation with the percentage of ventilation defects and the number of defects per slice found in asthma with a higher treatment burden. It also detects improvement in inhomogeneity with treatment that cannot be detected by other methods. |
| Bronchoscopy | It allows differential diagnosis with other abnormalities that simulate or coexist with severe asthma. Used with BAL, it increases the performance in the diagnosis of bacterial infection. It allows the diagnosis of inflammatory cell patterns, endobronchial, and molecular inflammation that is related to severe asthma with increased use of corticosteroids or worse lung function. |
MRI: magnetic resonance imaging; BAL: bronchoalveolar lavage
Genetic markers, biomarkers, lung function, radiological techniques, and BC are supportive tests and/or procedures for pediatric respiratory physicians to identify the endotype and/or phenotype of the child or adolescent with severe pediatric asthma.
Personalized medicine in severe pediatric asthma involves having the ability to understand the underlying mechanisms of the pathogenesis of each patient to initiate the most appropriate specific treatment for their disease. There are important limitations that must be considered when indicating these diagnostic studies in severe pediatric asthma. Firstly, the accessibility and cost of certain procedures are limited, requiring a rigorous selection process for eligible patients. The group of problematic severe asthmatics that have the greatest benefit from these studies is the STRA, which remains symptomatic despite maximum treatment and interventions in other modifiable factors. Likewise, another limitation that must be considered is the intricacy of carrying out the different studies. For example, performing a blood count to quantify EOs has a low degree of complexity, unlike others such as genetic markers, which require a specialized laboratory or MRI with hyperpolarized noble gases, which must have a protocol and trained personnel to administer the gas doses according to the expected lung capacity of each patient.
Despite all these limitations, diagnostic studies in severe pediatric asthma are useful in patients in whom it is necessary to know the phenotype/endotype, monitor disease activity, and select the treatment to reduce economic costs and/or adverse effects of unnecessary treatments. Ultimately, the development of diagnostic methods opens the way to improve the indication of existing therapies (e.g., biologicals) or the development of new therapies in the future.
129Xe: 129Xenon
A: artery diameter
ACT: Asthma Control Test
AT: air trapping
ATS/ERS: American Thoracic Society/European Respiratory Society
AUC: area under the curve
AWT%: percentage of airway wall thickness
BA: bronchus-artery
BAL: bronchoalveolar lavage
BC: bronchoscopy
BDR: bronchodilator response
BE: bronchiectasis
Bout: outer bronchial wall diameter
BWT: bronchial wall thickening
CoV: coefficient of variation
CT: computed tomography
DA: difficult asthma
EOs: eosinophils
FEF: forced expiratory flow
FeNO: fractional exhaled nitric oxide
FEV1: forced expiratory volume in 1 second
FVC: forced vital capacity
GINA: Global Initiative for Asthma
GINAq: Global Initiative for Asthma questionnaire
ICS: inhaled corticosteroids
IL-10: interleukin-10
ILCs: innate lymphoid cells
LAR: low attenuation regions
LCI: lung clearance index
miRNAs: microRNAs
MRI: magnetic resonance imaging
NGAL: neutrophil gelatinase-associated lipocalin
NRF2: nuclear factor erythroid 2-related factor 2
ppb: parts per billion
SAD: small airway dysfunction
sICAM-1: soluble intercellular adhesion molecule-1
STRA: severe treatment-resistant asthma
Th: T helper
TLRs: toll-like receptors
TSLP: thymic stromal lymphopoietin
VDP: ventilation defect percentage
AV: Writing—original draft, Writing—review & editing, Validation, Conceptualization. The author read and approved the submitted version.
The author declares that there are no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.