




Editor's Picks
Open Access
Original Article
Health literacy: application of SAHLPA-18 in patients with acute coronary syndrome
Aim:
To evaluate the health literacy (HL) of patients with acute coronary syndrome (ACS) admitted to a public hospital of high complexity in the interior of Minas Gerais, Brazil, through the application of the instrument Short Assessment of Health Literacy for Portuguese Speaking Adults (SAHLPA)-18.
Methods:
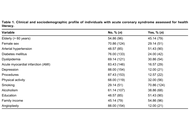
Retrospective cross-sectional study, from the Good Clinical Practices (GCP) project developed in a tertiary hospital. The 175 patients with ACS were analyzed, in which the profile and the SAHLPA-18 were evaluated.
Results:
It was found that 55.43% (97 among 175; 95% CI: 48.07–62.79) were considered with inadequate HL, and 40.00% of patients who have completed elementary school or higher education had inadequate HL (36 among 90). Female sex and complete primary education or higher increased the HL, and diabetes decreased the HL.
Conclusions:
We observed low literacy even in the presence of formal education, which, combined with the presence of diabetes, may represent a risk to patients with ACS, highlighting the need for continuous health education in this group regardless of the profile.
Open Access
Review
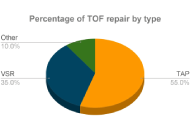
Comparison of transannular patch and valve-sparing repair techniques in tetralogy of Fallot
The aim is to evaluate the transannular patch (TAP) repair and valve-sparing repair (VSR) techniques following tetralogy of Fallot (TOF) correction, focusing on post-operative complications and cardiac function. A comprehensive search was performed in PubMed, EMBASE, and Scopus using relevant terms like “Tetralogy of Fallot, right ventricular outflow tract (RVOT), VSR, pulmonary valve replacement, transannular-patch repair”. Results indicated that VSR is favored due to its shorter cardiopulmonary bypass duration, preservation of the pulmonary valve, less demanding surgical requirements, shorter post-operative hospital stays, lower mortality rates, survival of at least 30 years, reduced pulmonary regurgitation, decreased right ventricular dysfunction, and improved physical activity tolerance and neurodevelopment. While TAP alleviates RVOT obstruction (RVOTO), it is associated with long-term pulmonary regurgitation. Both TAP and VSR are effective in managing TOF, but VSR provides better valve function preservation and long-term outcomes.
Open Access
Case Report
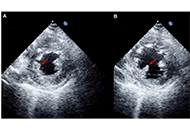
Challenges in diagnosing infective endocarditis in the context of recent COVID-19 infection: A case report
Infective endocarditis (IE) is a rare but potentially life-threatening condition with a wide spectrum of clinical presentations, often leading to diagnostic delay. The COVID-19 pandemic has added further complexity by overlapping clinical features and imposing constraints on diagnostic pathways. We report the case of a 48-year-old male who presented with prolonged non-specific symptoms following a recent COVID-19 infection. Multiple emergency department visits resulted in an initial diagnosis of viral illness. Subsequent clinical deterioration prompted further evaluation, which revealed severe aortic regurgitation due to a large aortic valve vegetation on transthoracic echocardiography. Blood cultures grew α-haemolytic Streptococcus mitis fulfilling the modified Duke criteria for IE. The patient developed complications, including heart failure and peripheral arterial embolisation, necessitating urgent surgical aortic valve replacement. This case highlights the diagnostic challenges of IE in the context of recent COVID-19 infection, where overlapping symptoms and altered healthcare pathways may contribute to delayed recognition. Clinicians should maintain a high index of suspicion for IE in patients presenting with persistent or atypical symptoms following COVID-19 infection. Early recognition and prompt intervention are essential to prevent serious complications.

Articles
Latest
Most Viewed
Most Downloaded
Most Cited
Open Access
Original Article
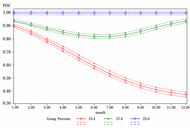
Statin adherence patterns among older adults on triple therapy: a real-world study using group-based trajectory model
Samuel C. Ofili ... Susan Abughosh
Published: June 09, 2026 Explor Cardiol. 2026;4:1012110
Open Access
Review
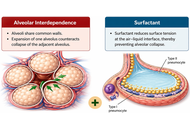
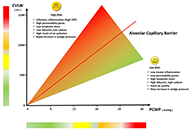
Cardiopulmonary interaction during spontaneous breathing and mechanical ventilation
Angel Benjamin Rojas ... Juan Carlos Vergottini
Published: May 12, 2026 Explor Cardiol. 2026;4:1012109
Open Access
Mini Review
Multiparity in women + cardiovascular disease: a South Asian perspective
Fatima Farrukh ... Zainab Samad
Published: May 12, 2026 Explor Cardiol. 2026;4:1012108
This article belongs to the special issue Cardiovascular Risk for Mothers and Offspring Resulting from Complicated Pregnancy

Open Access
Original Article
Prognostic trends of malignant cardiac tumors: insights from the Surveillance, Epidemiology, and End Results (SEER) registry
Riya Mehta ... Talal Asif
Published: May 05, 2026 Explor Cardiol. 2026;4:1012107

Open Access
Mini Review
Role of multimodality imaging in diabetic patients undergoing vascular bypass surgery: a narrative review
Nasir Yaqoob ... Amna Batool Aslam
Published: April 29, 2026 Explor Cardiol. 2026;4:1012106

Open Access
Review
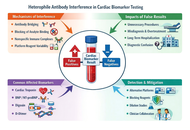
Heterophile antibody interference in cardiac biomarker testing: mechanisms, pitfalls, and clinical consequences
Ömer Burak Çelik ... Yusuf Karavelioğlu
Published: April 24, 2026 Explor Cardiol. 2026;4:1012105
Open Access
Review
Why and when should be lipoprotein(a) level measured?
Miłosz Broncel, Marlena Broncel
Published: December 29, 2023 Explor Cardiol. 2023;1:180–192
This article belongs to the special issue Common cardiovascular target for a wide gamut of contemporary health problems – thrombotic and arrhythmic sides of an inflammatory coin

Open Access
Review
Comparison of short-term and long-term effects of peroral L-carnitine intake: clinical implications of elevated TMAO levels in cardiovascular complications
Harsahaj Singh Wilkhoo ... Adnan Akhtar Shaikh
Published: February 10, 2025 Explor Cardiol. 2025;3:101250

Open Access
Review
Oxidized low-density lipoproteins and their contribution to atherosclerosis
Abdullatif Taha Babakr
Published: January 17, 2025 Explor Cardiol. 2025;3:101246
This article belongs to the special issue Molecular Mechanisms of Cardiovascular Aging

Open Access
Review
B-lines by lung ultrasound in cardiology
Marco Antonio Rodrigues Torres, Natália Moraes de Quevedo
Published: November 14, 2024 Explor Cardiol. 2024;2:265–279
This article belongs to the special issue Multimodality Imaging in Ischemic Heart Disease
Open Access
Review
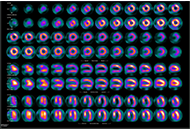
Diagnostic modalities for ischemic heart disease: evaluating the role of stress echocardiography, cardiac CT, and myocardial perfusion scintigraphy in guiding coronary angiography
Marco Fabio Costantino ... Luisiana Stolfi
Published: January 13, 2025 Explor Cardiol. 2025;3:101243
This article belongs to the special issue Multimodality Imaging in Ischemic Heart Disease
Open Access
Review
Echocardiographic Management of papillary muscle rupture during acute myocardial infarction
Paolo G. Pino ... Federico Nardi
Published: January 10, 2025 Explor Cardiol. 2025;3:101242
Open Access
Review
Diagnostic modalities for ischemic heart disease: evaluating the role of stress echocardiography, cardiac CT, and myocardial perfusion scintigraphy in guiding coronary angiography
Marco Fabio Costantino ... Luisiana Stolfi
Published: January 13, 2025 Explor Cardiol. 2025;3:101243
This article belongs to the special issue Multimodality Imaging in Ischemic Heart Disease
Open Access
Review
Oxidized low-density lipoproteins and their contribution to atherosclerosis
Abdullatif Taha Babakr
Published: January 17, 2025 Explor Cardiol. 2025;3:101246
This article belongs to the special issue Molecular Mechanisms of Cardiovascular Aging
Open Access
Editorial
Who is a reviewer? The Good, the Bad, and the Ugly phenotypes
Eugenio Picano
Published: January 23, 2025 Explor Cardiol. 2025;3:101248

Open Access
Review
Echocardiographic Management of papillary muscle rupture during acute myocardial infarction
Paolo G. Pino ... Federico Nardi
Published: January 10, 2025 Explor Cardiol. 2025;3:101242
Open Access
Review
Comparison of short-term and long-term effects of peroral L-carnitine intake: clinical implications of elevated TMAO levels in cardiovascular complications
Harsahaj Singh Wilkhoo ... Adnan Akhtar Shaikh
Published: February 10, 2025 Explor Cardiol. 2025;3:101250
Open Access
Original Article
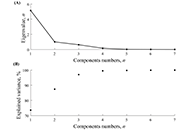
Heart rate variability in soccer players and the application of unsupervised machine learning
Wollner Materko ... Carlos Alberto Machado de Oliveira Figueira
Published: January 10, 2025 Explor Cardiol. 2025;3:101241
This article belongs to the special issue Exploring Exercise Cardiology: from Molecules to Humans
Open Access
Review
Laboratory markers of metabolic syndrome
Filipa Morgado ... Leonel Pereira
Published: June 24, 2024 Explor Cardiol. 2024;2:114–133
This article belongs to the special issue Molecular Mechanisms of Cardiovascular Aging
Open Access
Editorial
Who is the author: genuine, honorary, ghost, gold, and fake authors?
Eugenio Picano
Published: May 13, 2024 Explor Cardiol. 2024;2:88–96

Open Access
Review
Noninvasive identification and therapeutic implications of supernormal left ventricular contractile phenotype
Yi Wang, Lixue Yin
Published: June 17, 2024 Explor Cardiol. 2024;2:97–113

Open Access
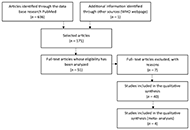
Systematic Review
Long-term cardiovascular sequelae of COVID-19 in patients with pre-existing heart failure: a systematic review
Razieh Parizad ... Bishav Mohan
Published: January 04, 2026 Explor Cardiol. 2026;4:101284

Open Access
Review
Oxidized low-density lipoproteins and their contribution to atherosclerosis
Abdullatif Taha Babakr
Published: January 17, 2025 Explor Cardiol. 2025;3:101246
This article belongs to the special issue Molecular Mechanisms of Cardiovascular Aging
Open Access
Review
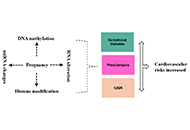
Epigenetic mechanisms linking pregnancy complications to cardiovascular disease in offspring
Kazim Raza Talpur ... Muhammad Waleed Abdullah
Published: November 07, 2024 Explor Cardiol. 2024;2:241–252
This article belongs to the special issue Cardiovascular Risk for Mothers and Offspring Resulting from Complicated Pregnancy
Special Issues
Ongoing Special lssues
Completed Special lssues
Periodontitis and cardiovascular disease: local and systemic links
Guest Editor: Gaetano Isola
Submission Deadline: December 31, 2026
Published Articles: 0
Heart–Brain Interactions: Clinical-Psychological Perspectives on Cardiovascular Function
Guest Editors: Pasquale Caponnetto; Graziella Chiara Prezzavento
Submission Deadline: August 15, 2026
Published Articles: 0
The Effect of Sexual Dysfunctions, Peripheral Artery Disease, and Patient Education on the Cardiovascular Risk in Diabetes
Guest Editors: Carmine Gazzaruso; Adriana Coppola
Submission Deadline: August 31, 2026
Published Articles: 1
Exploring Exercise Cardiology: from Molecules to Humans
Guest Editor: Paulo Gentil
Submission Deadline: August 31, 2026
Published Articles: 3
Cardiovascular Risk for Mothers and Offspring Resulting from Complicated Pregnancy
Guest Editor: Ilona Hromadnikova
Submission Deadline: August 31, 2026
Published Articles: 4
Molecular Mechanisms of Cardiovascular Aging
Guest Editor: Andrea Borghini
Submission Deadline: August 31, 2026
Published Articles: 5
Membership




Journal Information
Journal Indexing
Journal Metrics
Speed


From Submission to First Decision: 3 days
From First Decision to Acceptance: 63 days
From Acceptance to Publication: 20 days
Article Usage (total)
Views: 598,464
Downloads: 15,138
Acceptance Rate
45.4%; 2025
74.3%; 2024
80%; 2023

 Title: Unravelling the interplaybetween #Harmattan wind andbaroreflex functions: implicationon environmental health andcardiovascular #pathophys
Title: Unravelling the interplaybetween #Harmattan wind andbaroreflex functions: implicationon environmental health andcardiovascular #pathophysFollow the Journal



