Original Article
Original Article

Affiliation:
1Sultan Qaboos Comprehensive Cancer Care and Research Center, University Medical City, Muscat 131, Oman
ORCID: https://orcid.org/0000-0002-2473-6544
Affiliation:
1Sultan Qaboos Comprehensive Cancer Care and Research Center, University Medical City, Muscat 131, Oman
2Faculty of Dentistry, Cairo University, Cairo 12613, Egypt
Email: a.kamel-1@cccrc.gov.om
ORCID: https://orcid.org/0000-0002-3562-1099
Explor Cardiol. 2024;2:280–290 DOI: https://doi.org/10.37349/ec.2024.00040
Received: October 03, 2024 Accepted: November 01, 2024 Published: November 25, 2024
Academic Editor: Rochelle Buffenstein, Calico Life Sciences, University of Illinois Chicago, USA
The article belongs to the special issue Environmental Cardiology
Aim: This study aimed to assess oral health’s influence on COVID-19 outcomes in recovered individuals with pre-existing cardiovascular conditions.
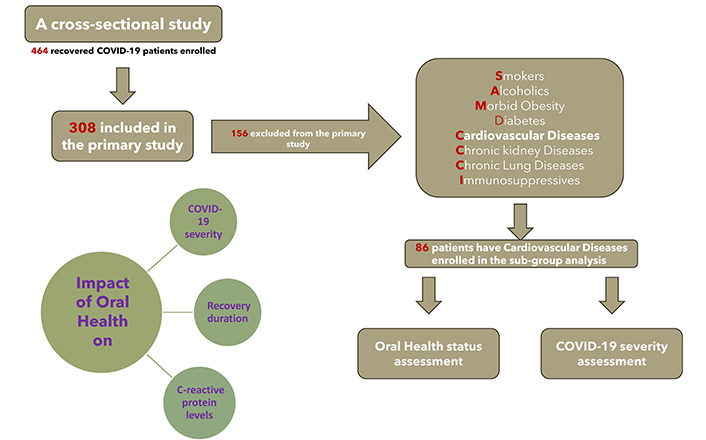
Methods: In the main study employing a cross-sectional design based on a questionnaire survey, 464 Egyptian patients who had recovered from COVID-19 were enrolled, with 86 individuals who had pre-existing cardiovascular conditions included in a subgroup analysis. Oral health was classified as poor and good based on scores from an 18-question survey with higher scores indicating better health. Severe COVID-19 was defined by criteria that included elevated respiratory and heart rates, severe dyspnea low oxygen saturation, high fever, and need for hospitalization or ICU care. Participants’ recovery duration was classified into three groups: fast (≤ 2 weeks), intermediate (4 weeks), and delayed (6 weeks), characterized by symptom-free status. Moreover, C-reactive protein (CRP) levels (> 18 mg/L) were considered elevated.
Results: Our results revealed that cardiac patients with poor oral health showed a significant association with severe COVID-19 cases, elevated CRP levels (> 18 mg/L), and a prolonged recovery period (6 weeks) (p < 0.001). In contrast, participants demonstrating good oral health were associated with milder COVID-19 cases, lower CRP levels, and faster recovery (p < 0.001).
Conclusions: Our findings indicate a significant link between the condition of oral health and the experienced severity of COVID-19 in cardiac patients. Poor oral health was associated with elevated CRP levels, delayed recovery, and more severe symptoms. These results highlight the importance of good oral hygiene as a modifiable factor in reducing infection severity, especially in vulnerable cardiac populations.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the virus accused of causing coronavirus disease 2019 (COVID-19). The World Health Organization (WHO) officially classified COVID-19 as a global pandemic on March 11, 2020 [1]. COVID-19 exhibits a wide range of symptoms, from mild flu-like manifestations to severe pneumonia that can progress to adult respiratory distress syndrome (ARDS), which has a mortality rate reaching up to 50%. In certain situations, a hyperactive immune response, referred to as “cytokine storm syndrome,” occurs leading to the release of harmful levels of cytokines such as TNF, IL-6, and IL-1β. This can cause vascular permeability and damage to organs like the kidneys and heart, with severe cases also reporting vascular complications [2].
The oral cavity hosts a diverse microbial population, including more than 700 different bacterial species. Viral infections in the respiratory tract can make individuals more vulnerable to secondary bacterial infections, leading to more severe illness. Studies have shown a significant association between COVID-19 severity and elevated viral load of SARS-CoV-2 detected in the oral cavity. Several mechanisms explain how oral bacteria could contribute to respiratory infections, including aspiration of pathogens into the lungs, facilitation of colonization by periodontal disease-associated enzymes, plaque harboring of pulmonary pathogens, and cytokine release from untreated periodontal disease altering respiratory epithelium. The presence of the transmembrane protein ACE2 (angiotensin-converting enzyme 2), a receptor for SARS-CoV-2, in oral tissues suggests that the oral cavity could serve as a reservoir for the virus, leading to high viral loads. These suggest a hypothesis that maintaining good oral health and reducing oral microbial load could potentially mitigate the severity of COVID-19 by reducing secondary respiratory infections and viral replication in the oral cavity [3, 4].
The oral cavity’s bacterial overgrowth in individuals with poor oral health can lead to bacteraemia, promoting chronic and acute inflammatory reactions. Periodontitis elevates tissue concentrations of proinflammatory cytokines, contributing to tissue damage and systemic effects [5]. Moreover, periodontitis may induce C-reactive protein (CRP) production in the liver, exacerbating inflammation. Elevated CRP levels in patients with severe COVID-19 could be associated with poor oral health, amplifying inflammatory cytokine production [6].
Recent studies have highlighted the link between oral health and various systemic conditions, including cardiovascular diseases and respiratory illnesses [7]. Moreover, several pieces of research have shown the positive impact of practising good oral hygiene in reducing susceptibility to acute viral respiratory diseases [8]. Moreover, the WHO and the Centers for Disease Control and Prevention (CDC) have recognized several risk factors accompanying severe COVID-19, such as aging, diabetes, hypertension, immunodeficiency, and cardiovascular diseases [2].
Individuals with pre-existing cardiovascular conditions make up a substantial portion of those with symptomatic COVID-19 infection and unfortunately tend to experience significantly poorer outcomes, with up to a tenfold increase in mortality. Pre-existing cardiovascular issues emerge as one of the most prominent predisposing factors to COVID-19 infection, heightening the risks of adverse outcomes and cardiovascular complications. Among patients admitted to hospitals with both COVID-19 and underlying cardiac conditions, the prognosis is poor, characterized by elevated mortality rates, occurrences of septic shock, and thromboembolic events [9, 10]. Inflammatory activation likely plays a significant role in patients with cardiac diseases, contributing to their susceptibility to COVID-19 and poorer clinical outcomes. Moreover, the infection is initiated by the viral spike protein binding to the ACE2 receptor, with ACE2 expressed predominantly in lung and heart tissues [11, 12].
Additionally, there is growing interest in the relationship between oral health and cardiovascular diseases, with evidence suggesting that poor oral health, particularly inflammatory conditions, may contribute to the development and progression of cardiovascular diseases [13, 14]. Given this background, this study aimed to provide valuable insights into this complex relationship by examining the intricate relationship between oral health and the severity of COVID-19 infections in individuals with preexisting cardiovascular conditions who have recovered.
In the main study of 464 patients who recovered from COVID-19, a subgroup analysis was conducted on 86 individuals with pre-existing cardiovascular conditions (Figure 1). These 86 recovered COVID-19 Egyptian patients with known coronary artery diseases participated in a cross-sectional study conducted via a questionnaire survey. Participants were selected from the COVID-19 dashboard records kept by the Egyptian Ministry of Health, covering the timeframe from April 1, 2020, to July 1, 2020. All individuals included in the study had confirmed COVID-19 diagnoses through polymerase chain reaction (PCR) testing. The study’s inclusion criteria encompassed individuals aged between 18 and 80 years, of any gender, who had tested positive for COVID-19 via PCR testing. Additionally, previously excluded from the main study, individuals with known pre-existing cardiovascular conditions were now included in a subgroup analysis. Pregnant patients, individuals receiving immunosuppressive drugs, and those with immunosuppressive diseases or severe chronic lung diseases were excluded from the study.
Cardiovascular conditions are defined as coronary artery disease [patients who had a history of coronary artery stenting or a history of cardiac surgery with bypass grafts or a history of myocardial infarction or Cardiac Care Unit (CCU) admission due to acute coronary syndrome or diagnosed as chronic coronary syndrome].
A questionnaire was administered to gather demographic information, including gender, age, weight, height, level of education, pre-existing cardiovascular conditions, and general health status, cardiac risk factors or chronic lung diseases (Supplementary material 1). The questionnaire comprised two sections: The first section assessed oral health status (Supplementary material 2), conducted by a panel of dentists analysing the answers and put oral health score for each patient. The questionnaire underwent expert review by a committee from Cairo University, including dental clinicians, physicians, and professors. It drew inspiration from Levin et al.’s 2013 study [15], known for its accuracy in caries risk assessment, and Prado et al.’s 2017 questionnaire [16], renowned for its reliability in evaluating oral health. Incorporating questions from both sources, the questionnaire design maintained a similar scoring system for assessing oral health status [15, 16].
While scoring and interpretation of COVID-19 severity were conducted using a questionnaire and hospital medical records (Supplementary material 3), overseen by a team of physicians.
Questionnaires were discussed through interviews conducted via phone calls, and participants were provided with a link to the questionnaire on Google Drive via WhatsApp message. The responses from both sections were carried out in a blinded manner.
All questions related to oral health status were incorporated into the current questionnaire, as referenced in Kamel et al., 2021 [17].
The main objective of our study was to assess how oral health conditions affect the severity of COVID-19 in cardiac patients. To accomplish this, we utilized a scoring system for oral health assessment, which comprised an 18-question questionnaire. Each response in the questionnaire was assigned a specific score, allowing for a comprehensive evaluation (Supplementary material 2). Total scores ranged from zero to 37, with higher scores indicating better oral health status. Participants were categorized into two groups: those with poor oral health (scores 0–18) and those with good oral health (scores 19–37).
Scoring and interpretation of COVID-19 severity were conducted using a questionnaire and hospital medical records that categorized patients into mild and severe cases (Supplementary material 3). Severe COVID-19 was defined by criteria such as a respiratory rate over 30 breaths per minute, heart rate above 100 beats per minute, significant dyspnea or chest pain, oxygen saturation below 93%, and a high fever above 39°C. Patients requiring hospitalization, oxygen supplementation, or admission to the intensive care unit (ICU) were classified as severe cases [18, 19].
CRP levels within the first week of COVID-19 infection were retrospectively obtained for each patient by retrieving laboratory test results from the questionnaire and cross-referencing them with medical records. Following this, the inflammatory marker’s levels were analysed with both COVID-19 severity and the oral health status of each patient.
Participants were categorized according to their recovery duration, characterized by the full symptoms’ resolution of symptoms, into three groups: fast recovery (within 2 weeks), intermediate recovery (4 weeks), and delayed recovery (6 weeks). Data collected from the questionnaire were then analysed to explore potential correlations between recovery duration, COVID-19 severity, and each participant’s oral health status.
Categorical variables were summarized as frequencies and percentages, while continuous variables were expressed as means with standard deviations (SD). Group comparisons were performed using the Chi-squared test for categorical data and the unpaired t-test for continuous variables between two groups. A significance level of p < 0.05 was set to indicate statistical significance. Furthermore, Spearman’s rank correlation coefficient (Spearman’s rho) was employed to assess correlations between comparison groups.
The study sample comprises 86 patients with documented coronary heart diseases who were initially excluded from the main study but subsequently included for subgroup analysis.
The statistically non-significant p-values for age, sex, smoking, diabetes, hypertension, dyslipidaemia suggest a balanced distribution of these demographic data and clinical variables across both groups (Table 1).
Participant demographics and clinical variables
| Clinical and demographic data | Poor oral health | Good oral health | p-value |
|---|---|---|---|
| Age (mean ± SD) | 62 ± 8.5 | 55.28 ± 7.8 | 0.08 |
| BMI (mean ± SD) | 27.8 ± 4 | 27.18 ± 4.3 | 0.4 |
| Gender (N) | |||
| Male | 22 | 48 | |
| Female | 6 | 10 | |
| High education level (N, %)(Bachelor’s, Master’s & PhD degrees) | 25 (89%) | 55 (95%) | |
| Diabetes (N, %) | 5 (18%) | 13 (22%) | 0.938 |
| Hypertension (N, %) | 6 (21%) | 15 (26%) | 0.325 |
| Dyslipidemia (N, %) | 7 (25%) | 16 (28%) | 0.791 |
| Chronic kidney disease (N, %) | 1 (4%) | 3 (5%) | 0.977 |
BMI: body mass index
The occurrence of severe COVID-19 cases significantly increased among cardiac patients with poor oral health (p < 0.001), whereas those with good oral health showed a significantly lower prevalence of severe COVID-19 illness (p < 0.001). The 95% confidence interval (CI) for this difference was between 0.42 and 0.77 (Table 2).
Evaluation of the influence of oral health on COVID-19 severity among cardiac patients (primary outcome)
| Oral health status | COVID-19 severity | p-value | |
|---|---|---|---|
| Severe | Mild | ||
| Poor (N, %) | 21 (75%) | 7 (25%) | < 0.001* |
| Good (N, %) | 9 (15.5%) | 49 (84.5%) | |
Group contrasts were evaluated utilizing the Chi-squared test for incidence comparisons. * A significance level of p < 0.05 was utilized as the criterion for statistical significance
Cardiac patients with severe COVID-19 demonstrated a significantly higher prevalence of elevated CRP levels (> 18 mg/L) compared to those with mild COVID-19 (p < 0.001). Conversely, individuals with mild COVID-19 exhibited notably reduced CRP levels (< 18 mg/L) (p < 0.001). Additionally, a statistically significant correlation was observed between elevated CRP levels and severe COVID-19 in patients with poor oral health (Spearman’s rho correlation coefficient, r = –0.885, p-value < 0.001). Similarly, a statistically significant correlation was found between CRP levels and mild COVID-19 in patients with good oral health (Spearman’s rho correlation coefficient, r = –0.397) (Tables 3, 4).
Evaluation of the oral health condition and COVID-19 severity influence on recovery duration and CRP levels in cardiac patients (secondary outcomes)
| Recovery duration & CRP outcomes | COVID-19 severity | p-value | Oral health status | p-value | |||
|---|---|---|---|---|---|---|---|
| Severe | Mild | Poor | Good | ||||
| Recovery duration | 6 weeks (N) | 17 | 3 | < 0.001* | 9 | 6 | < 0.001* |
| 4 weeks (N) | 6 | 13 | 5 | 16 | |||
| 2 weeks (N) | 7 | 40 | 14 | 36 | |||
| CRP | More than 18 (N) | 21 | 13 | < 0.001* | 19 | 11 | < 0.001* |
| Less than 18 (N) | 9 | 43 | 9 | 47 | |||
Group contrasts were evaluated utilizing the Chi-squared test for incidence comparisons. * A significance level of p < 0.05 was utilized as the criterion for statistical significance
Correlations between oral health condition and COVID-19 severity, recovery time, and CRP measurements
| Oral health & COVID-19 outcome | Rho | |
|---|---|---|
| Recovery duration | CRP value | |
| Oral health status | –0.449** | –0.885** |
| COVID-19 severity | –0.834** | –0.397** |
** The correlation is considered statistically significant (p-value < 0.001, Spearman’s rho correlation coefficient)
The prevalence of a prolonged recovery duration (6 weeks) was significantly higher among cardiac patients who experienced severe COVID-19 in relation to those with milder cases (p < 0.001). Conversely, individuals with mild COVID-19 demonstrated a significantly shorter recovery period (2 weeks) compared to their counterparts with severe illness (p < 0.001) (Table 3). Additionally, the occurrence of a prolonged recovery duration was significantly elevated among cardiac patients with compromised oral health status (p < 0.001). Whereas those with good oral health demonstrated a significantly quicker recovery period (p < 0.001) (Tables 3, 4).
Multivariate analysis was conducted to assess the independent association of various factors with severe COVID-19 outcomes. Poor oral health emerged as a significant independent predictor of severe COVID-19 (OR = 3.5, CI = 1.8–6.7, p < 0.001), indicating an increased likelihood of severe illness in cardiac patients with poor oral health. Other factors, including age, BMI, diabetes, hypertension, dyslipidaemia, and chronic kidney disease, did not show statistically significant associations (Table 5).
Multivariate analysis of factors associated with severe COVID-19 in cardiac patients
| Variable | Odds ratio (OR) | 95% confidence interval (CI) | p-value |
|---|---|---|---|
| Oral health (Poor vs. Good) | 3.5 | 1.8–6.7 | < 0.001 |
| Age | 1.1 | 0.98–1.3 | 0.09 |
| BMI | 1.5 | 0.91–1.2 | 0.3 |
| Diabetes | 1.2 | 0.6–2.3 | 0.92 |
| Hypertension | 1.1 | 0.6–2.1 | 0.33 |
| Dyslipidemia | 1.05 | 0.5–2.0 | 0.79 |
| Chronic kidney disease (CKD) | 1.3 | 0.3–2.8 | 0.98 |
In the current study, we aimed to evaluate the potential impact of oral health conditions on the severity of COVID-19 symptoms among patients with pre-existing cardiac conditions. This was accomplished through a comprehensive questionnaire and access to health records obtained from a national database, including blood test results. The dental portion of the questionnaire was evaluated independently by dentists unaware of the COVID-19 severity results, ensuring efforts to minimize bias.
The evaluation of COVID-19 severity has been somewhat ambiguous. However, several healthcare organizations such as the CDC, WHO, NHS, and NICE have utilized similar criteria to classify and evaluate COVID-19 severity, as employed in this study. However, many existing scoring systems relied on in-person consultations and examinations, which were not feasible during the pandemic due to restrictions on direct contact and certain examination methods. Some studies have demonstrated promising outcomes in assessing patients through alternative means such as phone and video call consultations, or electronic forms. Thus, a questionnaire designed to evaluate the severity of COVID-19 cases could be highly useful in such circumstances [20–22].
The present study involving cardiac patients found a significant association between COVID-19 symptoms severity and oral health. Specifically, poor oral health patients exhibited significantly heightened COVID-19 symptoms, while those with good oral health experienced a significant reduction in symptom severity (p-value < 0.001). These results underscore the possible influence of oral health on COVID-19 symptoms severity among individuals with cardiovascular diseases.
Four potential mechanisms could clarify how oral bacteria are involved in respiratory infections. Firstly, oral pathogens may enter the lungs through aspiration. Secondly, enzymes linked to periodontal disease could facilitate the attachment of respiratory pathogens to the airways. Thirdly, plaque may provide a favourable environment for the growth of pulmonary pathogens under specific conditions [23]. Lastly, untreated periodontal disease might lead to the continuous release of various cytokines, potentially modifying the respiratory epithelium and increasing susceptibility to respiratory pathogens [24].
Periodontopathic bacteria, including Fusobacterium, Prevotella, and Staphylococcus, were identified in the microbiome of individuals experiencing severe SARS-CoV-2 infections [25]. Additionally, bacterial superinfections were prevalent in severe COVID-19 cases, with over 50% of fatalities exhibiting bacterial superinfections [26].
Several studies have correlated COVID-19 severity with viral load, which is notably high not just in the nasal passages and nasopharynx but also in the oropharynx, rendering the oral cavity a significant reservoir of viral pathogens [27]. Research by Wölfel et al., 2020 [28] demonstrated SARS-CoV-2 actively replicating in the throat, especially within the initial 5 days of symptom onset, evidenced by the presence of viral RNA. This suggests the presence of actively infected cells in the specimens [28]. Therefore, effective oral hygiene practices and usage of oral germicides could potentially reduce viral multiplication, thereby not only mitigating disease dissemination but also impacting its severity and outcomes [29].
The existence of ACE2 in the oral cavity, heart and lungs suggests a potential association between oral health and COVID-19 severity, particularly in cardiac patients. ACE2 serves as the primary receptor for SARS-CoV-2, facilitating viral entry into cells. Since ACE2 is expressed in oral tissues, including the oral mucosa and salivary glands, the oral cavity may harbour the virus, leading to a higher viral load in saliva and crevicular fluid. In cardiac patients, who often have compromised cardiovascular health and may be using ACE inhibitors (ACEi), this interplay between oral health and COVID-19 severity is further emphasized. Thus, maintaining optimal oral health in cardiac patients could be critical in reducing SARS-CoV-2 transmission and mitigating COVID-19 severity. This underscores the importance of integrating oral health into overall health management, especially for those with pre-existing cardiac conditions [30].
As referenced in the main study by Kamel et al. [17], individuals with poor oral health status were found to have a 2- to 10-fold increase in bacterial colonization on teeth, leading to bacteraemia. Upon entry into the bloodstream, soluble antigens can interact with specific circulating antibodies, forming immunocomplexes that trigger several chronic and acute inflammatory reactions [17]. This association is further supported by several studies indicating that among patients hospitalized with COVID-19, diabetes, and cardiovascular disease—some of the most common comorbidities—there is a notable link between these conditions and periodontal disease [31].
In periodontitis, proinflammatory cytokines like gamma interferon, interleukins, prostaglandin E2, and TNF accumulate in tissues, contributing to tissue damage when the immune response becomes hyperactive. These cytokines stored in the periodontium can enter the bloodstream, causing systemic responses and influencing coagulation cascade and platelet aggregation [32]. Periodontitis, being an inflammatory condition, can trigger the liver to produce CRP. CRP binds to damaged cells, activates the complement system, and enhances the activity of phagocytes, including neutrophils [33].
The link between oral health and cardiovascular diseases has earned attention due to evidence suggesting that poor oral health, including conditions like periodontitis, could play a role in cardiovascular disease development and progression. Periodontitis, characterized by gum and tooth-supporting tissue inflammation, has been connected to higher risks of atherosclerosis and heart disease. The association’s underlying mechanisms entail the systemic dissemination of inflammatory mediators and oral bacteria, potentially exacerbating endothelial dysfunction and contributing to arterial plaque formation. Moreover, chronic oral inflammation may exacerbate systemic inflammation, affecting cardiovascular health. Given the significant role of cardiovascular diseases in COVID-19 severity, understanding the relationship between oral and cardiovascular health is crucial for assessing the influence of oral care on COVID-19 severity and recovery time [34–36].
In the current work, individuals with poor oral health experienced a significantly prolonged recovery (6 weeks). Whereas those who showed good oral health demonstrated a swifter recovery (p-value < 0.001), supporting the notion that oral health status significantly influences disease severity. However, it’s noteworthy that some participants with mild COVID-19 also experienced delayed recovery, possibly attributed to viral asthenia as indicated in existing literature.
CRP serves as a key inflammation marker, with elevated levels indicating a poorer prognosis in COVID-19 cases. Severe COVID-19 patients typically exhibit higher CRP levels than those with mild or moderate cases, with deceased patients often showing significantly higher values. Our study found a strong correlation between elevated CRP levels, COVID-19 severity, and poor oral health, suggesting an interplay between systemic inflammation and oral health status in cardiac patients [37, 38]. Although CRP is a non-specific marker influenced by various factors—including COVID-19 severity, immune dysregulation, and underlying cardiac disease—poor oral health may exacerbate systemic inflammation in this vulnerable group [39]. The cumulative effect of these factors, especially in cardiac patients predisposed to chronic low-grade inflammation, underscores the importance of addressing oral health alongside other contributing variables. Future research should control these variables to clarify the specific impact of oral health. Given the established prognostic significance of early CRP elevation in infections, incorporating oral health as part of comprehensive care may help manage inflammation and improve outcomes in cardiac patients with COVID-19 [36, 37].
Our study has several limitations, due to quarantine restrictions, the research team couldn’t conduct a dental examination and instead utilized an oral health questionnaire. Besides, the questionnaire did not cover factors like cytokine storm, vascular thrombosis and severity of cardiac conditions which can contribute to COVID-19 severity, requiring clinical examination, it did not cover more questions regarding the severity of coronary artery disease like angina score, severity of lesions, number of stents, methods of treatment divided to medical, interventional or surgical. Additionally, acquiring serial CRP values throughout the illness course for every participant was not feasible, although some studies suggest that CRP levels during the first week of illness may serve as a predictor of disease prognosis [36, 37]. Furthermore, subgroup analysis studies have limitations such as elevated false positives and intensified data-driven outcomes. Despite these constraints, this study identifies avenues for future research.
In conclusion, we observed that maintaining good oral health conditions could reduce the disease severity in this population. This observation was further reinforced by the correlation between oral health and CRP levels, where patients showing poor oral health exhibited significantly elevated CRP levels. Additionally, the recovery duration was notably deferred in individuals with poor oral health, indicating a potential association between oral health and the overall recovery process in cardiac patients with COVID-19. These findings highlight the significance of oral health as part of comprehensive care for cardiac patients, particularly during the COVID-19 pandemic. Additionally, this highlights the importance of maintaining good oral hygiene, not only for overall well-being but also as a potential modifiable factor in reducing the severity of infections, particularly COVID-19. These findings point to an intricate relationship between oral health, inflammation, and infection outcomes, especially in vulnerable cardiac patient populations.
ACE2: angiotensin-converting enzyme 2
COVID-19: coronavirus disease 2019
CRP: C-reactive protein
PCR: polymerase chain reaction
SARS-CoV-2: severe acute respiratory syndrome coronavirus 2
WHO: World Health Organization
The supplementary materials for this article are available at: https://www.explorationpub.com/uploads/Article/file/101240_sup_1.pdf.
AB: Conceptualization, Methodology, Formal analysis, Investigation, Visualization, Writing—original draft. AHMK: Conceptualization, Methodology, Formal analysis, Supervision, Validation, Writing—review & editing. Both authors read and approved the final manuscript.
Both authors confirm that they have no competing interest to disclose.
This questionnaire and methodology were approved by the Ethics Committee of Faculty of Dentistry, Cairo University, Cairo, Egypt, approval number: 21/6/20.
Informed consent to participate in the study was obtained from all participants.
Not applicable.
The data is available from the corresponding author upon reasonable request.
This research did not receive financial support from any funding agencies.
© The Author(s) 2024.
Copyright: © The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 2802
Download: 217
Times Cited: 0
Francesca Gorini, Alessandro Tonacci
Maria Grazia Andreassi