Who is a reviewer? The Good, the Bad, and the Ugly phenotypes
By offering their expertise, reviewers help authors improve their work and also support editors in selecting high-quality studies, thereby reinforcing the integrity of scientific literature. Much li
[...] Read more.
By offering their expertise, reviewers help authors improve their work and also support editors in selecting high-quality studies, thereby reinforcing the integrity of scientific literature. Much like in a Sergio Leone film, your manuscript encounters three possible types of reviewers on its editorial journey: the Good, the Bad, and the Ugly. The Good Reviewer is, for reasons unknown, favorably disposed toward both you and your manuscript. They find it “well-written, with literary and enjoyable style”, “original and timely”, and addressing a topic that is “scientifically and socially relevant”. Their comments are respectful, constructive, and focused on minor but meaningful improvements. Unfortunately, the Good Reviewer is as rare as a white unicorn; some researchers reach the end of their careers without ever encountering one, leading them to question their very existence. The Bad Reviewer is both bad at reviewing and a bad influence on your work. They reject your manuscript, but their reasons are vague and unconvincing. Their objections are often asinine, and when you respond thoroughly and decisively, they counter with even more nonsensical arguments. They may pressure you to cite irrelevant literature—often their work or that of their colleagues. In the end, your once-solid and cohesive manuscript emerges in a far worse state than the original. None of this would have been possible without the Bad Reviewer, who, unleashed by a negligent editor, exerts their detrimental influence on your article. The Ugly Reviewer appears with unsettling regularity—at least once a month. They believe your article is truly terrible, and often, they are right. The Ugly Reviewer, though harsh, is no fool. Their critiques are brutal and unforgiving, yet accurate. Years later, you may find yourself grateful to them for preventing you from publishing work that, in hindsight, would have irreparably tarnished your already modest scientific reputation.
Eugenio Picano
View:107
Download:6
Times Cited: 0
By offering their expertise, reviewers help authors improve their work and also support editors in selecting high-quality studies, thereby reinforcing the integrity of scientific literature. Much like in a Sergio Leone film, your manuscript encounters three possible types of reviewers on its editorial journey: the Good, the Bad, and the Ugly. The Good Reviewer is, for reasons unknown, favorably disposed toward both you and your manuscript. They find it “well-written, with literary and enjoyable style”, “original and timely”, and addressing a topic that is “scientifically and socially relevant”. Their comments are respectful, constructive, and focused on minor but meaningful improvements. Unfortunately, the Good Reviewer is as rare as a white unicorn; some researchers reach the end of their careers without ever encountering one, leading them to question their very existence. The Bad Reviewer is both bad at reviewing and a bad influence on your work. They reject your manuscript, but their reasons are vague and unconvincing. Their objections are often asinine, and when you respond thoroughly and decisively, they counter with even more nonsensical arguments. They may pressure you to cite irrelevant literature—often their work or that of their colleagues. In the end, your once-solid and cohesive manuscript emerges in a far worse state than the original. None of this would have been possible without the Bad Reviewer, who, unleashed by a negligent editor, exerts their detrimental influence on your article. The Ugly Reviewer appears with unsettling regularity—at least once a month. They believe your article is truly terrible, and often, they are right. The Ugly Reviewer, though harsh, is no fool. Their critiques are brutal and unforgiving, yet accurate. Years later, you may find yourself grateful to them for preventing you from publishing work that, in hindsight, would have irreparably tarnished your already modest scientific reputation.
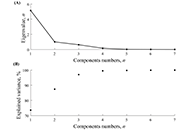 Heart rate variability in soccer players and the application of unsupervised machine learningOpen AccessOriginal ArticleAim: This study aimed to investigate the relationship between heart rate variability (HRV) parameters and performance in soccer players. Methods: This study used a cross-sectional design to [...] Read more.Wollner Materko ... Carlos Alberto Machado de Oliveira FigueiraPublished: January 10, 2025 Explor Cardiol. 2025;3:101241
Heart rate variability in soccer players and the application of unsupervised machine learningOpen AccessOriginal ArticleAim: This study aimed to investigate the relationship between heart rate variability (HRV) parameters and performance in soccer players. Methods: This study used a cross-sectional design to [...] Read more.Wollner Materko ... Carlos Alberto Machado de Oliveira FigueiraPublished: January 10, 2025 Explor Cardiol. 2025;3:101241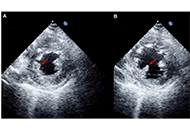 Echocardiographic Management of papillary muscle rupture during acute myocardial infarctionOpen AccessReviewPapillary muscle rupture is a rare but fatal complication of acute myocardial infarction. The incidence of this complication has been reduced to less than 0.1% of patients due to the advent of prima [...] Read more.Paolo G. Pino ... Federico NardiPublished: January 10, 2025 Explor Cardiol. 2025;3:101242
Echocardiographic Management of papillary muscle rupture during acute myocardial infarctionOpen AccessReviewPapillary muscle rupture is a rare but fatal complication of acute myocardial infarction. The incidence of this complication has been reduced to less than 0.1% of patients due to the advent of prima [...] Read more.Paolo G. Pino ... Federico NardiPublished: January 10, 2025 Explor Cardiol. 2025;3:101242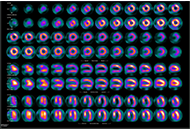 Diagnostic modalities for ischemic heart disease: evaluating the role of stress echocardiography, cardiac CT, and myocardial perfusion scintigraphy in guiding coronary angiographyOpen AccessReviewCardiovascular diseases, particularly ischemic heart disease (IHD), are the leading cause of mortality globally, accounting for 16% of deaths. Effective management of ischemic cardiomyopathy (ICM) i [...] Read more.Marco Fabio Costantino ... Luisiana StolfiPublished: January 13, 2025 Explor Cardiol. 2025;3:101243
Diagnostic modalities for ischemic heart disease: evaluating the role of stress echocardiography, cardiac CT, and myocardial perfusion scintigraphy in guiding coronary angiographyOpen AccessReviewCardiovascular diseases, particularly ischemic heart disease (IHD), are the leading cause of mortality globally, accounting for 16% of deaths. Effective management of ischemic cardiomyopathy (ICM) i [...] Read more.Marco Fabio Costantino ... Luisiana StolfiPublished: January 13, 2025 Explor Cardiol. 2025;3:101243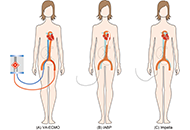 Implications of mechanical circulatory support devices in a pregnant woman with cardiogenic shockOpen AccessCase ReportData on the use of mechanical circulatory support devices in pregnant women are limited. A 27-year-old woman at 27 weeks and 6 days of gestation was supported by three different mechanical circulato [...] Read more.Johanna A. van der Zande ... Jerome M. J. CornettePublished: January 13, 2025 Explor Cardiol. 2025;3:101244
Implications of mechanical circulatory support devices in a pregnant woman with cardiogenic shockOpen AccessCase ReportData on the use of mechanical circulatory support devices in pregnant women are limited. A 27-year-old woman at 27 weeks and 6 days of gestation was supported by three different mechanical circulato [...] Read more.Johanna A. van der Zande ... Jerome M. J. CornettePublished: January 13, 2025 Explor Cardiol. 2025;3:101244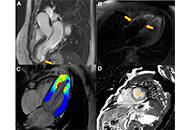 Takotsubo syndrome in the context of atherosclerotic acute myocardial infarction: the role of magnetic resonance imaging in determining cause or consequenceOpen AccessCase ReportWe present the case of a woman admitted for an acute ST-segment elevation myocardial infarction. Emergency catheterization was conducted, revealing diffuse lesions affecting 70% of the anterior desc [...] Read more.Cristhian Espinoza Romero ... Tatiana Torres LealPublished: January 14, 2025 Explor Cardiol. 2025;3:101245
Takotsubo syndrome in the context of atherosclerotic acute myocardial infarction: the role of magnetic resonance imaging in determining cause or consequenceOpen AccessCase ReportWe present the case of a woman admitted for an acute ST-segment elevation myocardial infarction. Emergency catheterization was conducted, revealing diffuse lesions affecting 70% of the anterior desc [...] Read more.Cristhian Espinoza Romero ... Tatiana Torres LealPublished: January 14, 2025 Explor Cardiol. 2025;3:101245 Oxidized low-density lipoproteins and their contribution to atherosclerosisOpen AccessReviewThe oxidation of lipoproteins has a key role in the development of atherosclerosis, a condition where plaque builds up in artery walls. Research shows that when low-density lipoprotein (LDL) oxidize [...] Read more.Abdullatif Taha BabakrPublished: January 17, 2025 Explor Cardiol. 2025;3:101246
Oxidized low-density lipoproteins and their contribution to atherosclerosisOpen AccessReviewThe oxidation of lipoproteins has a key role in the development of atherosclerosis, a condition where plaque builds up in artery walls. Research shows that when low-density lipoprotein (LDL) oxidize [...] Read more.Abdullatif Taha BabakrPublished: January 17, 2025 Explor Cardiol. 2025;3:101246 Association between a specific monocyte subset and heart failure with preserved ejection fraction in patients with uremiaOpen AccessOriginal ArticleAim: This study aimed to establish a model based on gene expression in peripheral blood mononuclear cells (PBMCs) for predicting the incidence of heart failure with preserved ejection fraction (H [...] Read more.Xinrui Wang ... Yang YangPublished: January 20, 2025 Explor Cardiol. 2025;3:101247
Association between a specific monocyte subset and heart failure with preserved ejection fraction in patients with uremiaOpen AccessOriginal ArticleAim: This study aimed to establish a model based on gene expression in peripheral blood mononuclear cells (PBMCs) for predicting the incidence of heart failure with preserved ejection fraction (H [...] Read more.Xinrui Wang ... Yang YangPublished: January 20, 2025 Explor Cardiol. 2025;3:101247 Who is a reviewer? The Good, the Bad, and the Ugly phenotypesOpen AccessEditorialBy offering their expertise, reviewers help authors improve their work and also support editors in selecting high-quality studies, thereby reinforcing the integrity of scientific literature. Much li [...] Read more.Eugenio PicanoPublished: January 23, 2025 Explor Cardiol. 2025;3:101248
Who is a reviewer? The Good, the Bad, and the Ugly phenotypesOpen AccessEditorialBy offering their expertise, reviewers help authors improve their work and also support editors in selecting high-quality studies, thereby reinforcing the integrity of scientific literature. Much li [...] Read more.Eugenio PicanoPublished: January 23, 2025 Explor Cardiol. 2025;3:101248