Review
Review

Affiliation:
Glycologic Limited, RG7 1PQ Reading, UK
Email: e.qi@glycologic.co.uk
ORCID: https://orcid.org/0000-0002-8274-5879
Explor Foods Foodomics. 2025;3:101065 DOI: https://doi.org/10.37349/eff.2025.101065
Received: July 22, 2024 Accepted: December 04, 2024 Published: January 16, 2025
Academic Editor: Luca Rastrelli, University of Salerno, Italy
The article belongs to the special issue Ketogenic Diet as Medical Nutrition Therapy
The so-called ‘ketogenic diet’ aimed to limit energy derived from carbohydrates, has many variations which cause confusion in the literature and beyond. For ‘intractable’ epilepsy (when seizures cannot be managed completely by drug therapy, also referred to as ‘refractory’, ‘uncontrolled’ or ‘drug-resistant’ epilepsy) the dietary fat to carbohydrate plus protein ratio is held at a ratio of 4:1 or 3:1. Thus promoting fat metabolism to ketone bodies as a primary energy source. This intervention limits glucose availability and consequently neural ‘excitability’ and seizures. Overall, the diet is high-fat, low-carbohydrate, and restricted protein in design. This generally accepted clinical approach (which is based on essentially fasting, historically) was applied and recorded back to the 1920s (for a patient with diabetic ketoacidosis). That observation (and others) initiated the diet applications for epilepsy and thereafter (or perhaps in parallel with) for both (i) weight management (especially the ‘Atkin’s diet) and (ii) enhanced sport performance. Products for weight loss tend to be high-fat but not in the ratios anticipated for seizure management, where, perhaps, brands have been developed that are more cognisant of consumer demands for desirable sensory characteristics than specific nutrient ratios. Whilst ketogenic type diets have been discussed in the context of different applications within the literature, the challenges associated with making and utilising ketogenic products for different applications/needs (with associated compliance) tend not to be addressed. This review addresses some of the challenges associated with creating and consuming ketogenic products, especially for seizure management, which restrict and control energy derived from carbohydrates. It aims to contextualise the issues faced with making and consuming this type of diet with significance generally to individuals interested in this approach to dietary energy regulation, most especially health professionals and people involved in sport nutrition.
Most people obtain macro- and micronutrients from a range of different foods according to their own preferences and socio-economic restraints. For some, however, the diet has to be restricted for health and performance related issues. The ketogenic diet is one such example where energy provision is switched deliberately from carbohydrate (and to some extent protein) to fat where the energy derived from dietary glucose (sugars, dextrin, and starch) ultimately is switched more to ketone bodies derived from fat metabolism. This is of particular importance to manage the neurological triggers for seizures although with considerable relevance to sport performance (as an alternative energy source to glucose and thus supporting the depletion of glycogen reserves) and weight management (with associated impact on blood glucose-insulin responses due to digestible carbohydrate consumption). This approach to dietary management thus has a considerable impact on relevant peoples’ lives, accessing and understanding relevant food sources and controlling their dietary habits accordingly. Many challenges are faced nutritionally and socially, as a consequence. Against this background, many articles are written about the diet but do not explain its contextual need, specific applications, and challenges. This review aims to highlight the physiological importance, purpose, and context of the diet and act as a meaningful reference source.
Dietary lipids (which are defined as organic compounds that are insoluble in water) are obtained from plant and animal sources. The relatively unsaturated nature of plant lipids, together with the absence of cholesterol makes them healthier in the diet than animal derived fats. The neutral lipids—mono-, di- and triglycerides of fatty acids esterified to glycerol, most especially as triglycerides, provide the bulk of dietary lipids (in excess of 95–97% is reported usually). The fatty acid chains may be of different lengths which are saturated, unsaturated, or polyunsaturated. Sterols, waxes, carotenoids, tocopherols, and terpenes are also classified as neutral lipids but tend to be sub-classified separately from the other neutral lipids. Polar lipids—especially phospholipids (although the category includes also glycolipids, sphingolipids, etc.) probably account for up to 2% of dietary lipids. The structure and classification of lipids have been discussed in detail by many authors elsewhere [1–7]. A useful eight-group lipid family classification system has been described by Fahy et al. [1, 2] as shown in Table 1. According to the British Nutrition Foundation [8] the dietary fat intake should not exceed (a total calorie intake per day of about 2,000 kcal for females and about 2,500 kcal for males depending on age etc.) 35% of total calories, (where saturated fat intake should not exceed 11% of total calories), representing approximately 30 g per day for men and 20 g for women. Similar data has been reported by Liu et al. [9] for other international organisations.
Lipid classification*
| Abbreviation | Group |
|---|---|
| FA | Fatty acyls |
| GL | Glycerolipids |
| GP | Glycerophospholipids |
| SP | Sphingolipids |
| ST | Sterol lipids |
| PR | Prenol lipids |
| SL | Saccharolipids |
| PK | Polyketides |
*: adapted from [1], CC BY
Their biological roles have been described in detail by others elsewhere [10]. The roles of lipids in/as foods are presented in Table 2. They are structural and provide the characteristic physical properties of many foods; which are very hard/impossible to replicate with other ingredients. In parallel, they provide sensory characteristics (especially mouthfeel) of foods too (cold, warm, and hot) which are often different eating experiences depending on processing (e.g., cheese in a sandwich versus melted cheese on a pizza). In addition to providing calories, essential fatty acids are required absolutely in the human diet. The fatty acids are major components of cell membranes, they can modulate gene transcription, act as molecular precursors (e.g., arachidonic acid conversion to prostaglandins), and provide energy [11]. At the macro-body level, it has been established with confidence over many years how they impact on physical aspects of the body (e.g., cancer, inflammation, arthritis, obesity, cardiovascular disease, skin structure, and mental health) as discussed by Glick and Fischer [11].
Roles and impacts of lipids in foods
| Characteristic | Role |
|---|---|
| Chemical | Potential source of rancidity and off-flavours due to oxidation |
| Physical | Structure |
| Bulk | |
| By interacting with other molecules, additional structural elements (e.g., complexing with carbohydrates) | |
| Carrier (with release control) of dissolved moieties (e.g., vitamins, colour, sweetness, flavour, and aroma) | |
| Coatings | |
| Emulsions (oil in water and water in oil) | |
| Cooking matrix (frying etc.) | |
| Responsive to thermal environment | |
| Sensorial | Mouthfeel |
| Flavour | |
| Encourage food consumption (perhaps excess) | |
| Physiological | Essential fatty acids critical for human tissues |
| Plant oils contain vitamin E | |
| Satiety | |
| Energy | |
| Animal fats associated with cholesterol content and impact on cardiovascular disease | |
| Contributes to obesity in excess |
Oxidation is a commonly experienced issue affecting fats (namely fatty acids) during storage, especially when not cooled or frozen. This rancidity process creates off-flavours which are not desirable and lead to food rejection/wastage. These off-flavours are often detectable with deshelled and packed nuts, where refrigerated storage can slow the process. Much has been written about the mechanisms of lipid oxidation [12] which has significant impact on food acceptability for both unprocessed and processed foods. These oxidation products are not passive in terms of health; that is their impact is more than sensorial. Kanner [13] for example indicated that after ingestion of oxidised fats both animals and humans excrete in the urine increased amounts of malondialdehyde (1,3-propanedial) and also lipophilic carbonyl compounds. Some of the oxidation products when absorbed from the gut seem to act as injurious chemicals which activate an inflammatory response. This is not only within the circulatory system but also in the digestive tract, liver, kidneys, and lungs. Kanner [13] indicated that the consumption of oxidised fat in the diet does, in fact, pose a chronic health threat. Malondialdehyde is both mutagenic and carcinogenic, reacting with deoxyribonucleic acid to form several types of adducts [14] which are discussed in detail elsewhere [15].
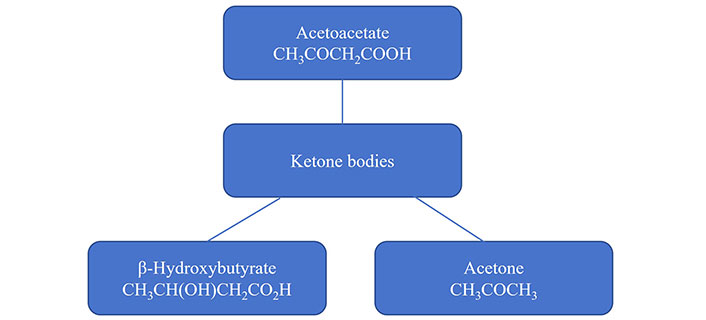
Kim [16] has discussed the origin of the so-called ‘ketogenic diet’ (ketone generating, high-fat, and low carbohydrate diet) developed by Dr. Russell Morse Wilder in the 1920s. Wilder’s work represents the first recorded application of the ketogenic diet for epilepsy management. The ketogenic diet utilisation for epilepsy management evolved in fact from a diabetic clinical case investigated/reported in 1922 (although, fasting type diets were developed in advance of the 1920s) as discussed additionally elsewhere [17–19]. The diet developed thereafter into sport applications gradually (key work in the 1980s [19]) with weight management applications in parallel [20]. The complementary low carbohydrate Atkin’s weight management/loss diet [21, 22] was actually initiated in the 1960s and 1970s (Table 3). The whole basis of the ketogenic dietary approach is to generate ketone bodies (Figure 1 and Table 4) from fat (fatty acid metabolism) for energy rather than using glucose as the primary energy source. Glucose reserves in the body (glycogen) are depleted rapidly (during work) compared to fat stores. This is the underlying mechanism considered desirable for optimal sport performance and weight management (Table 3, and discussed elsewhere in the text) by many. On the other hand, medically it is the neurological excitability role of glucose that is managed by a high lipid diet for epilepsy/seizures (Table 3); where ketone bodies are utilised by the brain instead for energy.
Low carbohydrate/ketogenic diet applications
| Application | Rationale | References |
|---|---|---|
| Cardiometabolic | Mixed effects on low-density lipoprotein cholesterol concentrations with some studies showing an increase. No clear evidence for advantages regarding effects on other cardiometabolic risk markers. May at the initiation of the diet (only) decrease blood pressure, triglyceride, and glycosylated haemoglobin concentration whilst increasing high-density lipoprotein. | [35, 74, 75] |
| Diabetes type 2 | Reduction in the use of medication in type 2 diabetes management. | [75] |
| Epilepsy | Manages epileptic seizures. | [76] |
| The low sugar high-fat diet alters synaptic neuronal excitability and neuro protection reducing trigger seizures. | [60, 77–79] | |
| Sport and endurance | Forces the body to use fat as a fuel source, which is more readily stored in larger depots than glycogen. | [19, 80–83] |
| Weight loss | May at the initiation of the diet (only) support weight loss. Not superior to other diets. | [20–22, 35, 74, 75, 80, 84] |
Ketone bodies*
| Common name | Alternative names |
|---|---|
| Acetoacetate | Acetoacetic acid, diacetic acid, 3-oxobutanoic acid |
| Acetone | Acetonum, dimethyl ketone, dimethyl carbonyl, ketone propane, β-ketopropane, propanone, 2-propanone, propan-2-one, and pyroacetic spirit |
| β-Hydroxybutyrate | 3-Hydroxybutyric acid, 3-hydroxybutanoic acid |
*: these molecules are generated in the liver from fatty acids (ketogenesis) during fasting, starving, as a consequence of the consumption of low carbohydrate diets, extreme exercise, excess consumption of alcohol, and due to unmanaged type 1 diabetes
There are actually a number of different formats (four essentially) of the original ketogenic (low carbohydrate/ketogenic) diet:
Original ‘long-chain triglyceride’ variant (4:1 or 3:1 fat:protein plus carbohydrate).
‘Medium-chain triglyceride’ variant, more appetible/flexible than (i) where the calorie intake is calculated based on the proportion of energy derived from the lipid, sometimes/often causes gastrointestinal side effects unfortunately.
‘Modified Atkins diet’—a more flexible approach than (i) or (ii), without strict intake construction or fat:non-fat ratio (1:1 to 4:1 probably), where the focus is really cutting out/down digestible carbohydrate (not protein) consumption.
‘Low glycaemic index’ [23, 24] approach where the glycaemic index reflects the rate and extent to which carbohydrates in a given food are digested and absorbed (as glucose), which in turn controls the blood glucose concentration.
These forms of diet are discussed in more detail elsewhere [18, 25–32].
Details about the ketogenic diet in terms of metabolism and impact on blood glucose control especially, may be found in a recent review by Qi and Tester [33]. This provides more information about the key ketone bodies generated as an energy source from lipid metabolism—acetoacetate, acetone, and β-hydroxybutyrate (Figure 1). Their alternative names are used often, too, as defined in Table 4. In terms of energy provision and impact, blood ketone concentrations above 0.5 mM represent a state of ‘nutritional ketosis’ where 3–5 mM can be achieved on the ketogenic diet [34].
It is very hard when reviewing the literature to come to a definitive position with respect to the long-term impact of the ketogenic diet on sport performance and weight loss [20]. Most success for the diet is reported on time-frames of up to (less than) one year [35]. Optimising sporting performance is a long-term commitment. According to Kaspar et al. [19] with respect to sport applications, low carbohydrate-high-fat and low carbohydrate ketogenic diets provide minimal benefit to athletes’ performance across different events. Harvey et al. [36] acknowledge that although ketogenic diets may result in undesirable side effects (such as altered blood lipid profiles, abnormal glucose homeostasis, increased adiposity, fatigue, and gastrointestinal distress) ketone body supplements can induce ketosis and as a consequence provide energy for exercise performance. The same authors indicate that the ketogenic diet provides a promising strategy to treat obesity, diabetes, and cardiac dysfunction whilst other authors see this potential less favourably. For weight loss, low carbohydrate diets are unlikely to produce significant long-term weight loss and in fact, may lead to serious health problems [37]. Seizure management control success due to consumption of the ketogenic diet is much better documented (discussed in more detail below).
High-fat (especially animal fat, with relatively high saturated fatty acid contents and presence of cholesterol) diets are associated with cardiovascular, diabetes, and cancer risks amongst others. It may be that a high plant-derived fat diet is altogether different in health outcomes than one rich in animal fats although that is not clear. The health debate concerning high-fat diet impacts on health has been reviewed in detail elsewhere [38, 39]. Although a high intake of dietary fats, especially saturated, has been linked to an increased risk of diabetes and cardiovascular disease the Mediterranean type-diet provides healthy monounsaturated fats which are apparently more effective in preventing cardiovascular mortality and coronary artery disease than low-fat, low-cholesterol diets [38]. The antioxidant and anti-inflammatory effects of these types of diets are potential mediators of these benefits [38].
Increasing the source of ketone bodies in the diet may be achieved by consuming a high-fat diet and by consuming the ketone bodies themselves. In recent years ketone body salts (for example calcium, magnesium, and sodium salts of 3-hydroxybutyrate) or specific lipid precursors of ketone bodies (e.g., medium chain triglycerides) have been added to nutrition/sport nutrition products directly (‘exogenous’ supply of the molecules). This approach is designed to drive upward the ketone concentration of the blood and thereafter ketone utilisation by the body. This area of nutrition research has been reviewed by many authors; although it is in its relative infancy [34, 40, 41]. No obvious detrimental health effects of eating these molecules at the concentrations used have been reported. In fact, four main exogenous routes of indirect/direct ketone body supply have been utilised in recent years [34, 42]:
Medium chain triglycerides (a mixture of 8 and 10 carbon fatty acids).
Ketone salts (as described above).
Ketone esters (made of β-hydroxybutyrate).
Direct consumption of β-hydroxybutyrate.
The calorific value of exogenous ketone bodies is approximately 4 kcal/g (17 kJ/g). However, according to Owen and Hanson [43], acetoacetate enters cells from either the (i) extracellular fluid or (ii) mitochondria, generated from β-hydroxybutyrate conversion by β-hydroxybutyrate dehydrogenase. This conversion in parallel, reduces nicotinamide adenine dinucleotide (NAD) to NADH. The β-hydroxybutyrate has a greater calorific content than acetoacetate of 4.5 kcal/g (19 kJ/g) versus 4 kcal/g (17 kJ/g). A comparison of this energy content is made with food macronutrients in Table 5. They are similar to digestible carbohydrate and protein in energy value.
Relative macronutrient calorie density compared to ketone bodies
| Nutrient | Energy in kcal/g | Energy in kJ/g |
|---|---|---|
| Fat | 9 | 38 |
| Alcohol | 7 | 29 |
| Protein | 4 | 17 |
| Carbohydrate | 3.75 | 16 |
| Dietary fibre | 2 | 8 |
| Ketone bodies | 4–4.5 | 17–19 |
One kilocalorie (1 kcal) is equivalent to 4.18 kilojoules (4.18 kJ)
Exogenous ketone consumption can certainly create ketosis [44]. According to many reports ketone bodies (such as the four exogenous forms described above) can in fact have a range of desirable therapeutic applications [29, 30, 35, 45]. One such application is cardiovascular disease as discussed by Yurista et al. [42]. They report that ketones (ketone bodies) can provide fuel for a failing heart, with a large range of other effects. These include improving endothelial function, ameliorating oxidative stress, improving mitochondrial function, exerting anti-inflammatory action, and mitigating cardiac remodelling. In addition, they report broad physiological impacts on body weight, blood pressure, glycaemia, and blood lipid profile. Takahara et al. [45] have described similarly the therapeutic benefits of ketone bodies during heart failure. Ketogenic metabolic therapy has been proposed for (breast) cancer [46]. In a recent review Neha and Chaudhary [47] discuss the ketogenic diet’s impacts on cancer more generally they indicate that the diet can augment the efficacy of conventional therapies by impacting on the ‘metabolic dynamics of cancer cells’. Diabetic benefits of a ketone generating/consuming diet are perhaps an obvious therapeutic option, in view of the reduced consumption of digestible carbohydrate and the associated impact on circulating insulin concentrations etc. [30], where ketogenic diets improve insulin sensitivity in particular [48]. Impacts on brain health are relevant too. Brain focussed ketone body therapy for diseases such as epilepsy, Alzheimer’s Disease, and psychiatric disorders have been discussed by Hashim and VanItallie [49] and Kovács et al. [50]. Apart from the many physical and psychiatric benefits of the ketogenic diet/ketones [30], there are also positive impacts on the body’s gut microbiome (profile) and more generally/systematically at the epigenome level of genetic expression [30]. Signalling roles of β-hydroxybutyrate link the outside environment to both gene regulation and cellular activity, relevant to a range of different human diseases and the aging process [51]. Whilst some authors [52] promote the long-term benefits of ketogenic diets for weight management in particular, where in parallel it decreases blood concentrations of triglycerides, low-density lipoprotein cholesterol, and blood glucose whilst increasing high-density lipoprotein cholesterol more recent reviews are not always as committed. Batch et al. [35] for example report that although the diet has a favourable impact on high-density lipoprotein cholesterol, there in fact a concomitant increase in low-density lipoprotein cholesterol and very-low-density lipoproteins which may lead to increased cardiovascular risks. Thus, further research is necessary to evaluate the long-term implications of the ketogenic diet according to these authors.
Aside from the health benefits of consuming the ketogenic diet discussed above, Crosby et al. [29] have indicated that although for most individuals the benefits outweigh risks, there are many risks consumers (of these types of diet) need to consider. For very low carbohydrate diets:
Increased exposure to low-density lipoprotein-cholesterol.
Potential neural tube defects in embryos/foetuses where women with restricted carbohydrate intake have been shown to be thirty percent more likely to give birth to a baby with anencephaly or spina bifida [53].
More broadly, because non-carbohydrate-based food consumption increases for high-fat diets, increased exposure to lipids and proteins may have positive and negative disease-causing impacts (depending largely on amount and frequency consumed), which include:
Alzheimer’s disease (some potential benefits).
Body weight (reduction potentially through carbohydrate-derived calorie limitation although may well be offset by increased fat-derived calories).
Cancer (some potential benefits of reducing glucose as an energy source for cancer cells).
Cardiovascular disease (potential for increased atherosclerosis risk).
Diabetes potential containment due to reduced consumption of dietary forms of glucose (although with some negative associated risks, potential ‘metabolic irregularities’ for type 1 where the benefits for type 2 are associated with short-term weight loss).
Kidney disease (potentially increased risk of kidney stones, high content of fruit and vegetables in the diet associated with low-fat dairy products carries the lowest risk for kidney stone formation according to Ferraro et al. [54]).
Non-alcoholic fatty liver disease (potential exacerbation, high-fat diet obesity associated link as discussed by Lian et al. [55]).
Wali et al. [38] have explored these issues—noting that ‘It is widely accepted that increased intake of fat, especially saturated fat, is a major driver of the increase in obesity and increased incidence of cardiometabolic disease.’ with further reference to EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA) [56] and Eckel et al. [57] in particular.
High-fat low-carbohydrate diets may exacerbate or cause hypercholesterolaemia in patients, be they with or without underlying genetic hyperlipidaemia [58]. These authors expanded their views further, especially for people with preponderance to dyslipidaemias, indicating that elevations of low-density lipoproteins with these diets does have the potential to create premature cardiovascular disease (especially with patients seeking to control their body weight).
With respect to epilepsy management, Williams and Cervenka [59] have also discussed the types of adverse effects of the diet on patients. These include:
Gastrointestinal effects (constipation, diarrhoea, and vomiting).
Weight loss.
An increase of lipids in the serum.
Overall, on one hand, essential fatty acids and unsaturated fatty acids are required/desirable in the diet, whilst on the other hand, saturated fatty acids and cholesterol are associated with poor health impacts [60–62]. They are all, regardless, providers of unnecessary calories if consumed in excess. Their major health-related aspects/impacts are highlighted in Figure 2. It is very important to avoid carrying excess body fat but retain a desirable body mass index (although the measurement does not reveal where the fat is, but acts as a general overview). See for example Nuttall [63]. Law [64] was very explicit about the risk of eating saturated fat: ‘Reducing dietary saturated fat by 7% of energy, a realistic target, would reduce serum cholesterol by 10% and mortality from ischaemic heart disease by 25–30%.’. Hence, it is critical when consuming a ketogenic type diet that an understanding of fat quality underpins the products consumed. Vegan focused products would provide a much healthier fat profile than fats derived from the majority of animal (including and perhaps especially dairy) related sources.
In terms of making high lipid content products for the ketogenic diet with a ratio of 3:1 or 4:1 of lipid:carbohydrates plus proteins [33], it is not an easy matter. Most food structure is imparted by proteins and carbohydrates. Trying to construct a structure that is not like liquid (oil) or solid (fat) requires a lot of skill and understanding of chemistry. Emulsions are an approach that has been used in some ketogenic diet approaches, but the solids content is obviously limited. Organoleptic properties need to be such that people will consume the products too, which will not happen if they are grossly undesirable.
In terms of marketed products that present themselves as ketogenic, there is really a medical and non-medical split:
Medical products—essentially emulsions or powders of ingredients that create a 3:1 or 4:1 ratio rigorously, targeted primarily at epilepsy management. It has proven to be very difficult for manufacturers to make other types of products with a higher fat content because of structure creating issues. A range of formats are offered by companies such as Abbott, Danone/Nutricia, and Nestlé/Vitaflo.
Sport and weight loss products—which are generally high-fat. Sometimes/usually low carbohydrate content too. Almost always without a 3:1 or 4:1 ratio; where the key sales angle is relatively high-fat, but without medical rigour constraints. Here the consumer takes sensory priorities much more critically than that might be expected for medical foods (although more modern medical foods are much better tasting than they were historically).
The problems associated with creating high-fat products are many, therefore, and can be defined (not exhaustively) as:
Structural integrity.
Retention of lipid during processing.
Retention of lipid post-processing.
Avoidance of lipid weep in packaging.
Lipid oxidation.
Easy of packaging.
Overall desirable sensory properties.
Compliance with ketogenic diets, especially for medical purposes, like all medical food diets, can be a challenge [26, 27, 32]. Apparently, although a classical ketogenic diet may be more effective in terms of impact, adults are more compliant with a modified Atkins (low-carbohydrate) diet [26]. Adherence and compliance of the ketogenic diet with epileptics are significant barriers to successful diet implementation [59]. Food choice and desirable characteristics are very important in human day-to-day life, it is not surprising that unless the diet is desirable, people are less compliant with the eating regime. It may be that compliance is enhanced for some individuals who consume processed foods, although this may not be beneficial even if the products are ketogenic, due to for example vitamin loss during processing.
The combined efficacy rates of all types of ketogenic diet, a classical ketogenic diet, and a modified Atkins diet are 42%, 52%, and 34% respectively with a corresponding combined compliance rate of 45%, 38%, and 56% according to Ye et al. [26]. Similar results have been presented by Kumar et al. [65]. These relatively low numbers are not perhaps surprising.
Mental health issues may benefit from the ketogenic diet (as mentioned above) although this is not altogether clear [66–71]. In this context, Adjibade et al. [72] went as far as to say (i) adherence to national dietary guidelines together with adequate nutrient intakes may be useful to prevent depressive symptoms through modifiable factors in the general population and (ii) diet in accordance with national or international guidelines may have beneficial effects with regard to mental health. Kumar et al. [65] reported that of patients who drop out of the classical ketogenic diet, 60% do due to psychosocial, fatigue, and weight loss reasons. With respect to the modified Atkin’s diet, almost half were discontinued due to inability to adhere. Overall, they report that where ketogenic diets are used to manage epilepsy, adherence is inversely related to the degree of dietary restriction with additional impacts of side effects and psychosocial stressors. The overall physiological impact of a ketogenic diet with time (alleviating inflammation and oxidative stress, modulating the gut microbiota, and improving metabolic health markers) can improve mental health disorders considerably [73]. In this context, the ketogenic diet may play potential role in the adjunctive treatment of serious mental disorders [73].
The ketogenic diet is an interesting, and perhaps a critical way for people with seizures, to fuel the body. Much hype has surrounded the diet for sport and weight loss applications where impacts are transitory. Slow/sustained/controlled energy release is probably useful within all the categories with calorie input control and exercise critical for weight management. The ketogenic diets will continue in favour of some groups no doubt involved in sport and weight control whilst new dietary variants pop up and become popular. The authors do believe that with better control of glucose availability to the brain (as in for example slowly digestible glucose containing polysaccharides) more control of seizures can be exerted [33]. The ketogenic approach in effect affiliated to this approach.
There are undoubted reasons why seizure control is managed by ketogenic diets. Glucose is as an energy source for patients with seizure tendencies, managed carefully to ‘dampen down’ its impact as a fuel for the brain and the metabolic consequences. This limits food choice and quality of life although there may be good reason to follow this diet. Issues of compliance with the diet do undoubtedly creep in. There is less compulsion to follow ‘ketogenic’ (which are essentially low carbohydrate) diets for sport performance and weight loss, especially when the impact is generally not sustained after one year. In terms of managing seizures where the consumption of a low carbohydrate diet is more critical than other applications, a high lipid content diet may be unhealthy if containing a high proportion of saturated fat and cholesterol (animal derived). Where dairy products have to be avoided due to the lactose content. Plant-derived foods tend to contain carbohydrates too, which creates additional limitations. Like any other medical food regime, adherence is critical and to support that end, it is very important that products are desirable to eat. To achieve this, very innovative approaches often need to be used to make them. This review considers the challenges of consuming ketogenic diets from a food choice and health perspective with relevance to food manufacturers and health professionals.
XQ: Writing—review & editing. RT: Writing—original draft. Both authors read and approved the submitted version.
Both authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

Giulia Izzo ... Mario Vitale
Leo Karl Hanke ... Paola Molettieri
Paola Pellegrini ... Maria D’Elia
Büşra Atabilen, Yasemin Akdevelioğlu
Alejandro Borrego-Ruiz, Juan J. Borrego