Original Article
Original Article

Affiliation:
1Instituto de Química y Fisicoquímica Biológicas (IQUIFIB), Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires, Buenos Aires 1113, Argentina
Affiliation:
2Department of Biosciences, Universidad Maimónides, Ciudad Autónoma de Buenos Aires, Buenos Aires 1405, Argentina
Email: felipe.inserra@gmail.com
Affiliation:
3Hospital de Alta Complejidad en Red El Cruce-Néstor Kirchner, Florencio Varela, Buenos Aires 1888, Argentina
Affiliation:
3Hospital de Alta Complejidad en Red El Cruce-Néstor Kirchner, Florencio Varela, Buenos Aires 1888, Argentina
Affiliation:
4Cátedra de Matemáticas, Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires, Buenos Aires 1113, Argentina
Affiliation:
3Hospital de Alta Complejidad en Red El Cruce-Néstor Kirchner, Florencio Varela, Buenos Aires 1888, Argentina
Affiliation:
2Department of Biosciences, Universidad Maimónides, Ciudad Autónoma de Buenos Aires, Buenos Aires 1405, Argentina
Affiliation:
5Centro de Estudios Biomédicos, Básicos, Aplicados y Desarrollo (CEBBAD), Universidad Maimónides, CONICET, Buenos Aires 1405, Argentina
Affiliation:
6Medical Clinic Section, Clínica Santa Isabel, Ciudad Autónoma de Buenos Aires, Buenos Aires 1406GZJ, Argentina
Affiliation:
7Medical Clinic Section, Hospital de Infecciosas Francisco Javier Muñiz, Ciudad Autónoma de Buenos Aires, Buenos Aires 1282AEN, Argentina
Affiliation:
7Medical Clinic Section, Hospital de Infecciosas Francisco Javier Muñiz, Ciudad Autónoma de Buenos Aires, Buenos Aires 1282AEN, Argentina
Affiliation:
7Medical Clinic Section, Hospital de Infecciosas Francisco Javier Muñiz, Ciudad Autónoma de Buenos Aires, Buenos Aires 1282AEN, Argentina
Affiliation:
8Cátedra de Inmunología, Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires, Buenos Aires 1113, Argentina
9Instituto de Estudios de la Inmunidad Humoral (IDEHU), CONICET-Universidad de Buenos Aires, Buenos Aires 1113, Argentina
Affiliation:
8Cátedra de Inmunología, Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires, Buenos Aires 1113, Argentina
9Instituto de Estudios de la Inmunidad Humoral (IDEHU), CONICET-Universidad de Buenos Aires, Buenos Aires 1113, Argentina
Affiliation:
1Instituto de Química y Fisicoquímica Biológicas (IQUIFIB), Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires, Buenos Aires 1113, Argentina
Email: marielagironacci@gmail.com
Affiliation:
10Instituto de Medicina y Biología Experimental de Cuyo (IMBECU), CONICET-Universidad Nacional de Cuyo, Mendoza 5500, Argentina
11Facultad de Ciencias Médicas, Universidad Nacional de Cuyo, Mendoza 5500, Argentina
Email: wmanucha@yahoo.com.ar; wmanucha@fcm.uncu.edu.ar
Explor Med. 2023;4:246–253 DOI: https://doi.org/10.37349/emed.2023.00137
Received: November 18, 2022 Accepted: February 04, 2023 Published: April 26, 2023
Academic Editor: Bernhard Ryffel, University of Orleans, France
The article belongs to the special issue Lung Fibrosis—Models and Mechanisms
Aim: To evaluate angiotensin II (Ang II) and Ang-(1-7) levels and the cytokine profile in patients hospitalized with mild coronavirus disease 2019 (COVID-19) and contrast them with patients with identical clinical conditions but treated with high doses of vitamin D (vitD).
Methods: From the 218 patients recruited (ClinicalTrials.gov NCT04411446), 16 participated in this sub-study and were randomized to a single oral dose of 500,000 IU vitD (n = 10) or placebo (n = 6). Plasmatic Ang II and Ang-(1-7) levels were determined by radioimmunoassay and interleukins (ILs) 1, 6, 8, and 10 and tumor necrosis factor alpha (TNF-α) by enzyme-linked immunosorbent assay before and after treatment. Parallel, serum 25-hydroxyvitamin D3 (25-OH vitD) concentrations as vitD status was measured by a chemiluminescence immunoassay.
Results: A trend towards an increase in Ang-(1-7) and a decrease in Ang II levels were observed in placebo- and vitD-treated COVID-19 patients compared to baseline values. There was no difference in Ang II and Ang-(1-7) levels between placebo- and vitD-treated COVID-19 patients. Similar results were obtained with ILs profile. COVID-19 patients showed an increase in the protective component of the RAS which was not improved by vitD treatment.
Conclusions: VitD did not improve RAS disbalance in COVID-19. Notwithstanding, the authors visualize that acute treatment with high doses of vitD may show a trend to a decline in inflammatory ILs and an increase in protective markers. Finally, the authors would like to highlight the limitations of this preliminary study, namely the small number of patients and the use of a large single bolus dose of vitD rather than lower daily doses for extended periods with prolonged follow-up times. All these factors need special consideration in the designs of new vitD supplementation trials. All these factors need special consideration in the designs of new vitD supplementation trials (ClinicalTrials.gov identifier: NCT04411446).
A low vitamin D (vitD) status is one of the most frequent factors associated with the severity of the incidence of coronavirus disease 2019 (COVID-19) and its serious complications [1], mainly associated with an overreaction of pro-inflammatory cytokines [2]. In this sense, vitD supplementation is an adequate strategy to reduce severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus infection and complications by modulating cytokines and moderating the inflammatory cascade.
Angiotensin-converting enzyme 2 (ACE2) metabolizes angiotensin II (Ang II) into Ang-(1-7) and acts as a receptor for SARS-CoV-2 [3]. ACE2 is sequestered by the virus, causing an imbalance in the axes of the renin-angiotensin system (RAS) [4]. Of interest, vitD suppresses the RAS/ACE/ACE2 axis and is therefore postulated as a possible treatment for COVID-19 disease attenuation; however, controversies exist regarding vitD in COVID-19 treatment [5].
Therefore, in CholecAlcifeRol to improveD (CARED-TRIAL) we tested the effects of single high-dose vitD (vitD3) supplementation on respiratory outcomes of hospitalized COVID-19-positive patients [6]. In addition, since some reports have shown that vitD favors the protective axis of the RAS, we hypothesized that COVID-19 patients treated with high doses of vitD would have their RAS balanced. Thus, we aimed to evaluate Ang II and Ang-(1-7) levels and cytokine levels in patients hospitalized with mild COVID-19 treated with high doses of vitD in a prespecified sub-study of the same clinical trial.
The Ethics Committee of the Hospital El Cruce (Comité de Ética en Investigación Hospital de Alta Complejidad El Cruce) approved the study on 23 June 2020 (reference 36/2020). The local ethics committees of the participating institutions approved the study protocol before the start of the trial in each site. The work described has been carried out in accordance with The Code of Ethics of the World Medical Association and with the principles of the Helsinki Declaration.
Patients enrolled in this sub-study came from two CARED-TRIAL (Identifier number NCT04411446) study sites. CARED-TRIAL was conducted in hospitalized patients with a SARS-CoV-2 confirmed infection and meets the criteria to enroll in The CholecAlcifeRol to improveD the outcomes of patients with COVID-19, a multicenter, randomized, double-blind, sequential, placebo-controlled trial, described previously [6]. Participants were ≥ 18 years old, of either gender, requiring hospitalization for at least 24 h, oxygen saturation ≥ 90% (measured by pulse oximetry), breathing ambient air, and with at least one of the following conditions: age 45 or older, hypertension, diabetes, chronic obstructive pulmonary disease or asthma (at least moderate), cardiovascular disease (history of myocardial infarction, percutaneous transluminal coronary angioplasty, coronary artery bypass grafting or valve replacement surgery) or body mass index (BMI) ≥ 30. Patients were randomly assigned in a 1:1 ratio to receive vitD as a single oral dose of 500,000 IU (10 patients) of soft gel capsules or a matching placebo (6 patients), given after randomization. Following the recommendation of the local health authorities, blood samples were not routinely taken from patients hospitalized for uncomplicated COVID-19, thus, serum levels of calcium, phosphorus, creatinine, and others were not determined. We only extracted blood samples from patients participating in the sub-study after they signed the informed consent.
Blood collection was performed under institutional review approval after informed consent. Blood samples were obtained the first day the patient was admitted to the general ward for hospitalization and 3 to 7 days after treatment (placebo or vitD). Whole blood was collected from 16 patients into ethylenediaminetetraacetic acid (EDTA)-containing tubes with protease inhibitors for Ang II and Ang-(1-7) measurement and a separate tube for 25-OH vitD (vitD status) and interleukins (ILs) measurement.
Serum 25-OH vitD concentrations were measured by chemiluminescence immunoassay as previously described [A98856, Access 25(OH) Vitamin D Total, Beckman Coulter Inc., USA] [7]. The laboratory is subject to standardization and external quality control assessment (Vitamin D Standardization-Certification Program by CDC).
Blood samples were collected in EDTA-tubes containing 0.44 mmol/L o-phenanthroline, 1 mmol/L Na+para-chloromercuribenzoate and 25 mmol/L EDTA. Samples were centrifuged at 3,000 xg for 20 min at 4°C and plasma were loaded into SepPak C18 cartridges for angiotensins extraction as previously described [8]. Because angiotensin may not be completely extracted from the cartridge, angiotensin recovery was calculated and corrected for each sample. Angiotensin levels were quantified by radioimmunoassay using angiotensin labelled in our laboratory as previously described [9]. Limits of detection of Ang II and Ang-(1-7) assays were 4 pg/mL and 20 pg/mL, respectively. Intra-assay and inter-assay variability were 13.7% ± 2.3% and 12.4% ± 3.1%, respectively.
The ILs levels were measured by commercially available sandwich enzyme-linked immunosorbent assays (ELISAs) following manufacturer’s instructions. The following ELISA kits were employed: human IL-6 (BD Biosciences cat. 555220), human IL-8 (BD Biosciences cat. 555224), human IL-1β (BD Biosciences cat. 557953), human IL-10 (BD Biosciences cat. 555157), and human tumor necrosis factor alpha (TNF-α, BD Biosciences cat. 550610).
The data were analyzed by a statistician using SPSS Statistics 19 software. Kolmogorov–Smirnov test was applied to verify normal distribution, and Kruskal–Wallis test was utilized to investigate differences. Statistical analysis was performed on each group (baseline vs. after placebo treatment and baseline vs. after vitD treatment) with paired t-test. At the same time, the differences between groups after treatments were analyzed with an unpaired t-test. Baseline and achieved concentrations were compared for each laboratory variable using paired t-tests. A P < 0.05 was considered statistically significant.
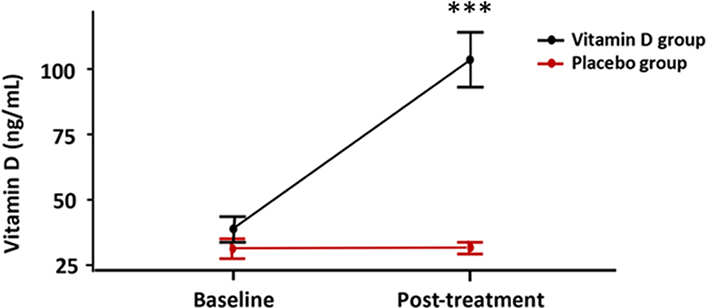
VitD supplementation significantly increased 3-fold serum vitD status (basal: 37.40 ± 4.92 vs. vitD-treated 106.7 ± 10.66 ng/mL), while there was no change in vitD status in the placebo-treated group (basal: 29.83 ± 3.43 vs. placebo-treated 30.50 ± 2.12 ng/mL). None of the 16 participants had evidence of vitD deficiency (Figure 1).
Since a cytokine storm characterizes COVID-19, we measured IL-6, IL-8, IL-1β, IL-10 and TNF-α in placebo- and vitD-treated COVID-19 patients. IL-1β and IL-8 were increased in placebo- and vitD-treated COVID-19 patients, respectively, compared to baseline values. We did not find changes in IL-6, IL-10 and TNF-α. There was no difference in cytokine levels between placebo- and vitD-treated COVID-19 patients. On the other hand, there was a trend toward increasing the serum level of IL-10 in the vitD-treated group (Table 1).
Serum levels of ILs and RAS components at baseline and post-treatment in placebo and vitD treated groups
| Serum levels of ILs and RAS components | Baseline vs. placebo treatment | Baseline vs. vitD treatment | Change from baseline vitD treated vs. placebo treated | |
|---|---|---|---|---|
| IL-6 (pg/mL) | BaselinePost-treatment | 19.9 ± 5.3 vs.17.6 ± 5.8 | 27.7 ± 8.8 vs.35.1 ± 21.0 | 7.4 ± 22.4 vs.−2.2 ± 4.1 |
| IL-8 (pg/mL) | BaselinePost-treatment | 17.9 ± 5.0 vs.17.4 ± 4.0 | 20.9 ± 3.4 vs.30.8 ± 16.3 | 9.8 ± 13.9 vs.−0.5 ± 6.1 |
| IL-1B (pg/mL) | BaselinePost-treatment | 6.3 ± 1.2 vs.7.5 ± 1.4 | 7.2 ± 0.8 vs.5.5 ± 0.4 | −1.7 ± 0.4 vs.1.2 ± 0.4 |
| TNF-α (pg/mL) | BaselinePost-treatment | 12.3 ± 2.4 vs.12.7 ± 3.7 | 12.6 ± 1.7 vs.9.0 ± 3.1 | −3.6 ± 3.0 vs.0.3 ± 3.1 |
| IL-10 (pg/mL) | BaselinePost-treatment | 29.2 ± 3.8 vs.31.4 ± 7.2 | 35.6 ± 7.1 vs.63.7 ± 35.9 | 28.1 ± 35.5 vs.2.2 ± 6.0 |
| Ang-(1-7) (pg/mL) | BaselinePost-treatment | 851.2 ± 130.8 vs.1014.4 ± 170.3 | 645.3 ± 68.5 vs.977.9 ± 190.1 | 332.6 ± 148.2 vs.163.1 ± 55.7 |
| Ang-II (pg/mL) | BaselinePost-treatment | 209.0 ± 43.9 vs.81.0 ± 21.3 | 132.2 ± 24.2 vs.86.9 ± 27.5 | −45.2 ± 19.5 vs.−128.0 ± 26.0 |
| Ang-(1-7)/Ang-2 | BaselinePost-treatment | 2.5 ± 0.3 vs.8.6 ± 2.3 | 5.2 ± 1.2 vs.17.7 ± 4.7 | 12.5 ± 3.7 vs.6.0 ± 2.2 |
Changes from baseline. The results are shown as mean ± standard error mean (SEM). * P < 0.05; ** P < 0.01
Regarding plasmatic Ang II and Ang-(1-7) levels, there was an increase in Ang-(1-7) and a decrease in Ang II levels in placebo- and vitD-treated COVID-19 patients compared to baseline values. There was no difference in Ang II and Ang-(1-7) levels between placebo- and vitD-treated COVID-19 patients (Table 1).
The ratio of Ang-(1-7)/Ang II as a surrogate marker of ACE2 activity was higher in placebo- and VitD-treated COVID-19 patients compared to baseline values. However, this ratio was not different between placebo- and VitD-treated COVID-19 patients (Table 1).
In an exploratory analysis excluding patients with BMI greater than 40 and those older than 70, in the remainder, there was a tendency for a higher reduction of pro-inflammatory cytokines among the patients receiving vitD (data not shown).
The present study showed that vitD was given to hospitalized subjects with mild to moderate COVID-19 and did not influence Ang-(1-7) and Ang II levels as well as ILs levels. To our knowledge, this is the first report that showed Angs levels in COVID-19 patients treated with vitD.
The patients have shown no significant differences between the placebo- and vitD-treated groups on the primary outcome (change in the respiratory sepsis-related organ failure assessment score), not even on secondary outcomes [6]. Although supplementation with a high dose of vitD increased its serum level more than three times, this treatment did not prevent respiratory worsening. The possible reasons for these contrasting findings are consistent with a previous review that highlighted complex factors such as varying doses, duration, the timing of vitD, vitD type, administration, patient populations, sample sizes, and differences in the criteria for defining the severity of COVID-19, among others [5]. In this sense, the bolus dose of vitD, the vitD status at baseline, pharmacologic treatment (corticosteroids), and the patient’s clinical condition were determinant factors for present results. In the other studies with a similar design, acute administration of high doses of vitD in moderate or severe COVID-19 has also shown similar results; moreover, recently a systematic review arrived at the same conclusion [10].
Regarding the potential mechanistic participation of RAS and the production of cytokines, the present study’s main findings showed a significant increment in the serum levels of Ang-(1-7) and Ang-(1-7)/Ang II ratio in vitD-treated patients. The placebo-treated group also had an increment in these variables but was smaller than that of vitD-treated patients.
The patients treated with vitD achieved an impressive increment in vitD status between days 3 and 7 after supplementation (Figure 1). Unexpectedly, their mean baseline values were around 30 ng/mL in both placebo- and vitD-treated groups. None of the participants had a serum level of less than 20 ng/mL (vitD deficiency), which probably influenced the results.
Regarding cytokines, the results did not show significant differences in the basal levels between the groups, nor were differences between the post-treatment groups (Table 1). However, although it was not statistically significant, serum levels of IL-10—an anti-inflammatory marker increased by 85% in those treated with vitD vs. 10% in the placebo group.
It is essential to consider that obesity and aging are two leading factors fulling the chronic inflammatory process [11]. Therefore, we performed an exploratory analysis, excluding patients (with BMI greater than 40 and those older than 70); in the remainder, there was a greater reduction of pro-inflammatory cytokines among the patients receiving vitD (P < 0.05).
On the other hand, it is known that the balance between the levels of the enzymes ACE and ACE2, appropriate ACE2 activity, and Ang-(1-7) levels might be decisive in preventing immune-induced damage and making certain pulmonary tissue repairs [12]. In this regard, the results have shown promising findings. The Ang-(1-7) increases more in the vitD-treated group (51% than in the control group (19%), although without significant differences between groups (Table 1).
The relationship between vitD and RAS interaction was established 20 years ago when Li and colleagues demonstrated, among other findings, that renin secretion is suppressed by vitD [13]. Regarding the vitD/RAS interaction and the participation of the ACE2/Ang-(1-7) signaling pathway, it has been found that vitD acts as a cofactor in the attenuation of heart disease by inhibiting the RAS [14]. Furthermore, restoring normal vitD status in patients with hypovitaminosis D leads to blockade of the peripheral RAS [15]. Additionally, calcitriol has been found to modulate altered upregulation of hepatic RAS in conditions of insulin resistance [16]. Therefore, a low vitD status is associated with increased renin synthesis, resulting in the overactivation of RAS and increased production of Ang-II, and vice versa [17]. VitD deficiency has also been shown to result in the overexpression of angiotensin-converting enzymes (ACE and ACE2) [18].
Furthermore, lung studies have shown that vitD, through its receptors, attenuates acute lung injury by blocking the RAS [19]. While if vitD deficiency is chronic, in that case, uncontrolled overactivation of the RAS can induce pulmonary fibrosis [20]. A robust relationship between vitD deficiency and mortality in older adults before and during the COVID-19 pandemic has been proved, specifically this study concludes that severe vitD deficiency (< 10 ng/mL) is an independent predictor of mortality or severe vitD deficiency can be quite fatal [21]. In addition, a recent nonlinear Mendelian randomization analysis concluded a causal relationship between vitD deficiency and mortality [22]. In the same way, a meta-analysis of 25 RCTs confirmed that patients with low vitD status gained more protection with the supplementation [23]. Therefore, these patients could be targeted for vitD treatment because they have a higher potential benefit [24]. Overall, our findings agree with the current evidence that positive COVID-19 patients with adequate vitD status evolve positively.
Finally, we would like to highlight the limitations of this preliminary study, namely the small number of patients, and the use of a large single bolus dose of vitD rather than lower daily doses for extended periods with prolonged follow-up times. All these factors need special consideration in the designs of new vitD supplementation trials.
This trial failed to demonstrate a significant decrease in inflammatory cytokines with oral vitD supplementation. The increase in vitD status was associated with a downward trend in pro-inflammatory cytokines and an improvement in anti-inflammatory markers. However, these results need to be confirmed in trials with a more significant number of patients since the low number of patients enrolled, the severity of the disease in the patients, and the higher-than-usual vitD status at enrollment may have affected the results.
ACE2: angiotensin-converting enzyme 2
Ang II: angiotensin II
BMI: body mass index
CARED-TRIAL: CholecAlcifeRol to improveD
COVID-19: coronavirus disease 2019
EDTA: ethylenediaminetetraacetic acid
ILs: interleukins
RAS: renin-angiotensin system
SARS-CoV-2: severe acute respiratory syndrome coronavirus 2
TNF-α: tumor necrosis factor alpha
vitD: vitamin D
MGS and EMC: Data curation. FI and WM: Conceptualization, Formal analysis, Funding acquisition, Writing—original draft, Writing—review & editing. JM, LA, and CT: Funding acquisition, Investigation, Methodology. MN: Software, Validation. LF: Funding acquisition. PIFI, FR, MSC, MB, and GdL: Investigation, Methodology. DHGM: Data curation, Formal analysis. MMG: Conceptualization, Formal analysis, Writing—original draft, Writing—review & editing.
The authors declare that they have no conflicts of interest.
This study has been carried out in accordance with The Code of Ethics of the World Medical Association and with the principles of the Helsinki Declaration. Research Ethics Committee from Hospital de Alta Complejidad El Cruce approved this study.
Informed consent to participate in the study was obtained from all participants.
Not applicable.
All datasets generated/analyzed for this study are included in the manuscript.
This work was supported by grants from the Research and Technology Council of Cuyo University (SECyT), Mendoza, Argentina, and from ANPCyT FONCyT, both of which were awarded to Walter Manucha (Grant no. IP-COVID-19-931). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2023.
Copyright: © The Author(s) 2023. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

Paolo Giannoni ... Daniela de Totero
Lena B. Kim, Anna N. Putyatina