Original Article
Original Article

Affiliation:
1Department of Clinical Pathology, Faculty of Medicine, Universitas Sriwijaya–RSUP Dr. Mohammad Hoesin, Palembang 30126, Indonesia
Email: pheyliana@fk.unsri.ac.id
ORCID: https://orcid.org/0000-0002-2081-180X
Affiliation:
2Medical Profession Program, Faculty of Medicine, Universitas Sriwijaya, Palembang 30114, Indonesia
ORCID: https://orcid.org/0009-0005-4216-8260
Affiliation:
1Department of Clinical Pathology, Faculty of Medicine, Universitas Sriwijaya–RSUP Dr. Mohammad Hoesin, Palembang 30126, Indonesia
ORCID: https://orcid.org/0009-0009-3465-2991
Affiliation:
3Department of Internal Medicine, Faculty of Medicine, Universitas Sriwijaya–RSUP Dr. Mohammad Hoesin, Palembang 30126, Indonesia
ORCID: https://orcid.org/0000-0001-9010-285X
Affiliation:
4Department of Clinical Pathology, Faculty of Medicine, Universitas Sriwijaya, Palembang 30114, Indonesia
ORCID: https://orcid.org/0000-0001-9557-467X
Affiliation:
3Department of Internal Medicine, Faculty of Medicine, Universitas Sriwijaya–RSUP Dr. Mohammad Hoesin, Palembang 30126, Indonesia
ORCID: https://orcid.org/0000-0002-1732-7435
Affiliation:
5UCL Centre for Nanotechnology and Regenerative Medicine, Division of Surgery and Interventional Science, University College London–Royal Free Hospital, NW3 2PS London, UK
ORCID: https://orcid.org/0000-0001-6975-8096
Explor Med. 2023;4:839–846 DOI: https://doi.org/10.37349/emed.2023.00181
Received: April 03, 2023 Accepted: August 07, 2023 Published: October 31, 2023
Academic Editor: Marcos Roberto Tovani-Palone, Saveetha Institute of Medical and Technical Sciences (SIMATS), India
The article belongs to the special issue Emerging Infectious Diseases
Aim: Coronavirus disease 2019 (COVID-19) is a respiratory infection caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The SARS-CoV-2 has undergone several mutations, and ultimately, Indonesia was designated the Asian epicenter of the pandemic in 2021 due to the emergence of Delta variant SARS-CoV-2. Therefore, this study aimed to determine the characteristics of the Delta variant SARS-CoV-2 gene mutations.
Methods: This is a cross-sectional descriptive study to determine the mutation characteristics of the Delta variant SARS-CoV-2 with data collected from patients’ medical records and whole genome sequencing (WGS).
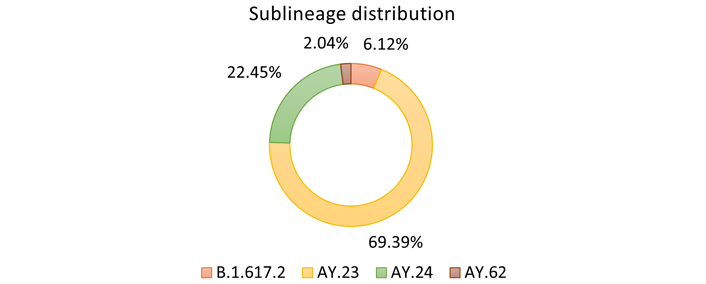
Results: The forty-nine patients who contracted the Delta variant SARS-CoV-2 were mainly aged 31−45 years and female. Four sublineages were identified, namely AY.23 (69.39%), AY.24 (22.45%), B.1.617.2 (6.12%), and AY.62 (2.04%), with fever and malaise being the most common clinical manifestations (79.60%). Furthermore, the spike (S) protein was most frequently mutated (12 mutations), with mutations in the Delta variant SARS-CoV-2 membrane (M) protein, nucleocapsid (N) protein, open reading frame (ORF), and nonstructural protein (NSP) also identified.
Conclusions: The most common Delta variant SARS-CoV-2 sublineage in the current study cohort was AY.23, with the S protein being most frequently mutated. Continuous genomic surveillance is required to contain future outbreaks or infection waves, especially during the COVID-19 pandemic.
Coronavirus disease 2019 (COVID-19) is a respiratory infection caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), first reported in Wuhan, China, in December 2019 [1]. The rapid spread of COVID-19 led to the World Health Organization (WHO) action to declare it a pandemic in March 2020 [2]. COVID-19 has been linked to more than 760 million cases and 6.9 million deaths worldwide as of May 31, 2023 [3]. This pandemic significantly hinders every aspect of human life, particularly in healthcare, social, economic, and education [4].
During the COVID-19 pandemic, frequent mutations in SARS-CoV-2 resulted in new variants with distinct characteristics. The mutation is distinguished by a shift in the SARS-CoV-2 spike (S) protein gene, leading to antigenic drift [5], which is a change in viral protein caused by virus gene mutations. This process is responsible for the reduced effectiveness of vaccinations and the host immunogenic responses. WHO categorized such variants as variants under monitoring (VuM), variants of interest (Vol), and variants of concern (VoC) [6]. One of the most considerable variants was the Delta variant, which led to a substantial increase in hospitalizations, intensive care unit (ICU) admissions, and deaths compared to the Alpha variant (original SARS-CoV-2) [7]. The Delta variant median case fatality rate (CFR) was 8.56%, significantly higher than the overall COVID-19 CFR of around 1.0% [7, 8]. Furthermore, due to increased positivity rate, bed occupancy, mortality, and medical care shortage (including oxygen) in the second half of 2021, Indonesia was designated as the COVID-19 epicenter in Asia [9].
In addition to monitoring the SARS-CoV-2 variant, WHO is working to prevent the disease by developing vaccines using various technologies. The COVID-19 vaccine platform is partitioned into four types: messenger ribonucleic acid (mRNA), viral vector, protein/peptide subunit, and inactivated virus [10]. As of February 2023, approximately 69.7% of the world’s population had received complete COVID-19 vaccination, with 74.45% of the population in Indonesia being vaccinated [11].
However, no research on the characteristics of the SARS-CoV-2 Delta variant gene mutation has been reported in Indonesia. Therefore, this study was conducted to determine the features of this mutation. This research is necessary to determine the sociodemographic, gene mutation types, and clinical manifestations of COVID-19 and provides epidemiological data especially relevant in the case of possible re-emergence of previously prevalent variants.
This study employed a descriptive observational cross-sectional design based on secondary data of COVID-19 patients treated in RSUP Dr. Mohammad Hoesin, Palembang, Indonesia (a tertiary-level hospital) between September and December 2021 (during the second wave of the outbreak in Indonesia) when the South Sumatera province reported 2,015 confirmed COVID-19 cases (https://dinkes.sumselprov.go.id/covid19-sumsel/). Furthermore, the sample of the confirmed Delta variant SARS-CoV-2 patients from RSUP Dr. Mohammad Hoesin for whole genome sequencing (WGS). The analysis was undertaken at the Eijkman Institute for Molecular Biology, Jakarta, Indonesia. This study was approved by the Sriwijaya University Faculty of Medicine Ethics Review Committee (approval number: 242-2022).
All patients treated during the study period were sampled, with patients who had a confirmed COVID-19 test result [reverse transcription polymerase chain reaction (RT-PCR)] and detectable WGS data included in this study. Patients with incomplete medical records and recurrent SARS-CoV-2 infections were excluded. In total, the data of 49 subjects with the Delta variant SARS-CoV-2 were analyzed using IBM SPSS Statistics for Windows, Version 24.0 (Armonk, NY: IBM Corp.) and Microsoft Excel 2016 (Redmond, WA: Microsoft Corporation). The data were presented descriptively in tables, figures, and narratives.
The sublineage distribution of the Delta variant SARS-CoV-2 in the observed COVID-19-positive cohort is shown in Figure 1. Most patients had the AY.23 sublineage (34; 69.39%), followed by AY.24 (11; 22.45%), B.1.617.2 (3; 6.12%), and AY.62 was found in only one patient (2.04%).
The patient characteristics presented in Table 1 revealed that most subjects (17; 34.69%) were between the ages of 31 and 45, with only three patients (6.13%) aged > 60 years. The cohort was mainly female (65.2%), with a female:male ratio of 1.88:1.
Patient characteristics
| Variable | Delta variant distribution | ||||
|---|---|---|---|---|---|
B.1.617.2 (n = 3; 6.12%) | AY.23 (n = 34; 69.39%) | AY.24 (n = 11; 22.45%) | AY.75 (n = 1; 2.04%) | Total (n = 49) | |
| Age | |||||
| 6–18 years | 0 (0%) | 1 (2.94%) | 3 (27.27%) | 0 (0%) | 4 (8.16%) |
| 19–30 years | 1 (33.33%) | 13 (38.24%) | 1 (9.09%) | 0 (0%) | 15 (30.61) |
| 31–45 years | 2 (66.67%) | 10 (29.41%) | 4 (36.36%) | 1 (100%) | 17 (34.69%) |
| 46–59 years | 0 (0%) | 8 (23.53%) | 2 (18.18%) | 0 (0%) | 10 (20.41%) |
| ≥ 60 years | 0 (0%) | 2 (5.88%) | 1 (9.09%) | 0 (0%) | 3 (6.13%) |
| Gender | |||||
| Male | 0 (0%) | 12 (35.29%) | 5 (45.45%) | 0 (0%) | 17 (34.69%) |
| Female | 3 (100%) | 22 (64.71%) | 6 (54.55%) | 1 (100%) | 32 (65.31%) |
| Vaccination status | |||||
| Unvaccinated | 1 (33.33%) | 9 (26.48%) | 1 (9.09%) | 1 (100%) | 12 (24.49%) |
| One dose | 1 (33.33%) | 4 (11.76%) | 3 (27.28%) | 0 (0%) | 8 (16.33%) |
| Two doses | 1 (33.33%) | 21 (61.76%) | 7 (63.63%) | 0 (0%) | 29 (59.18%) |
| Clinical manifestation | |||||
| Fever | 2 (66.67%) | 27 (79.41%) | 10 (90.91%) | 0 (0%) | 39 (79.60%) |
| Cough | 2 (66.67%) | 24 (70.59%) | 7 (63.63%) | 1 (100%) | 34 (69.39%) |
| Runny nose | 2 (66.67%) | 21 (61.76%) | 10 (90.91%) | 1 (100%) | 34 (69.39%) |
| Sore throat | 1 (33.33%) | 22 (64.71%) | 7 (63.63%) | 1 (100%) | 31 (63.27%) |
| Malaise | 3 (100%) | 27 (79.41%) | 9 (81.82%) | 0 (0%) | 39 (79.60%) |
| Fatigue | 2 (66.7%) | 21 (61.76%) | 6 (54.54%) | 0 (0%) | 29 (59.18%) |
| Abdominal pain | 0 (0%) | 7 (20.59%) | 2 (18.18%) | 0 (0%) | 9 (18.37%) |
| Diarrhea | 0 (0%) | 6 (17.65%) | 2 (18.18%) | 0 (0%) | 8 (16.33%) |
| Pneumonia | 0 (0%) | 7 (20.59%) | 2 (18.18%) | 0 (0%) | 9 (18.37%) |
| Anosmia | 0 (0%) | 14 (41.17%) | 6 (54.54%) | 0 (0%) | 20 (40.82%) |
| Ageusia | 0 (0%) | 12 (35.29%) | 1 (9.09%) | 0 (0%) | 13 (26.53%) |
| Shortness of breath | 1 (33.33%) | 14 (41.17%) | 4 (36.36%) | 1 (100%) | 20 (40.82%) |
| Nausea or vomiting | 1 (33.33%) | 15 (44.12%) | 3 (27.28%) | 0 (0%) | 19 (38.78%) |
| Severity | |||||
| Mild | 3 (100%) | 26 (76.48%) | 9 (81.82%) | 1 (100%) | 39 (79.60%) |
| Moderate | 0 (0%) | 4 (11.76%) | 1 (9.09%) | 0 (0%) | 5 (10.20%) |
| Severe | 0 (0%) | 4 (11.76%) | 1 (9.09%) | 0 (0%) | 5 (10.20%) |
The most prevalent clinical complaints were fever (39; 79.60%), malaise/lethargy (39; 79.60%), cough (34; 69.39%), and runny nose (34; 69.39%). Furthermore, most participants (79.60%) only had mild symptoms, while the proportions of moderate and severe manifestations were similar at 10.20%.
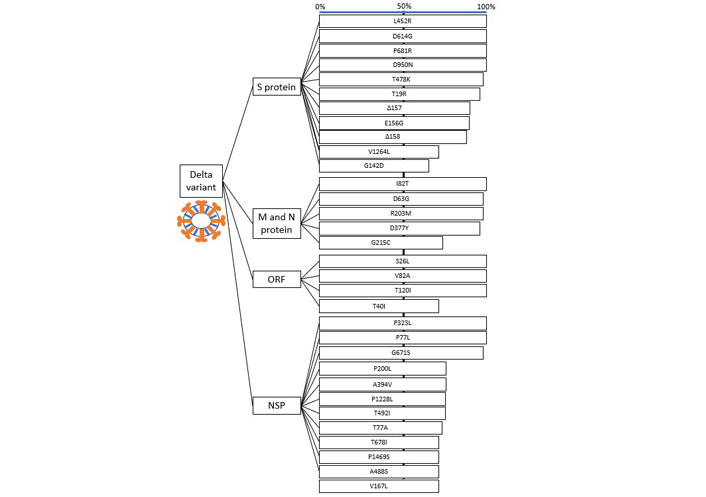
The mutations can be divided into four categories based on their locations: the S protein, the membrane (M) and nucleocapsid (N) proteins, the open reading frame (ORF), and the nonstructural protein (NSP). The most substantial mutation (> 50% of samples) was identified in at least two sublineages (Figure 2), with ten gene mutations in the S protein occurring in all Delta variant sublineages. Moreover, four mutations were found in all samples, namely L452R, D614G, P681R, and D950N. Other observed mutations included T478K (48; 97.96%), T19R (47; 95.92%), Δ157 (44; 89.80%), Δ158 (43; 87.76%), and E156G (44; 89.80%).
In contrast, there were several notable mutations in specific sublineages (> 50% occurrence): V1264L (AY.23), A222V, P104S, V1786L, and A446V (AY.24). The distribution of gene mutations in the M and N proteins was equivalent, and included I82T (49; 100%), D63G (48; 97.96%), R203M (48; 97.96%), and D377Y (47; 95.9%). A similar pattern was also observed for the ORF and NSP gene mutations, with the three ORF mutations: S26L, V82A, and T120I, occurring in all Delta variant sublineages. Meanwhile, three major NSP mutations were identified: P323L (49; 100%) and P77L (49; 100%) for NSP13, and G617S (48; 97.96%) for NSP12.
Four sublineages of the Delta variant SARS-CoV-2 were identified in the forty-nine COVID-19 patients at Dr. Mohammad Hoesin General Hospital, namely AY.23, AY.24, B.1.617.2, and AY.62. AY.23 is the main sublineage found in Indonesia during the Delta variant outbreak and was identified in 20.3% of the samples [12]. Meanwhile, the B.1.617.2 sublineage, known as the original Delta variant, was less common, similar to a study in Malaysia which found that B.1.617.2 was the most common variant at the start of the second wave of COVID-19 but declined over time and was eventually replaced by the AY.23 sublineage from September 2021 (the same study period as the current investigation) [13]. The AY.62 sublineage is not common in many Asian countries, including China and India, and originated primarily in North America (12% in the United States and Mexico). A Mexican study reported this sublineage in 224 of 18,097 COVID-19 patient samples (1.23%), primarily in southeastern Mexico [14].
The most frequent mutation observed in this cohort occurred in the S gene, with a total of eleven distinct mutations identified. These mutations, including the L452R, P681R, D614G, and T478K, were responsible for the enhanced transmissibility of the Delta variant SARS-CoV-2 [15]. D614G is the most common mutation in India (99.9%) and the United States (99.9%), followed by D950N, the second most common type observed, especially in the United States (98.3%) [16]. Furthermore, S protein mutations have a stabilizing effect, facilitating the binding of the S protein receptor-binding domain (RBD) with human angiotensin-converting enzyme 2 (ACE2). These mutations may be associated with higher infectivity, reduced sensitivity to neutralization, resistance to antiviral immunity elicited by vaccination, and weak interaction with antiviral medications [17]. However, this is not always the case because numerous mutations in the S gene destabilize antibody complexes while not affecting the receptor complex, offering an adaptive advantage through immune evasion [18].
In addition to the S protein mutation, all subsequent genetic sequence transformations increase the ability of SARS-CoV-2 to produce a sustained infection. The SARS-CoV-2 N mutation can enhance viral spread, fitness, and replication [19]. The three NSP mutations (P323L, G671S, and P77L) identified in our cohort were similar to those previously reported (P323L, M463I, P77L, G671S, and T125N) [20]. In addition, two mutations in the ORF region were similar to a previous study (ORF3, ORF7a, and ORF8), with ORF3 and ORF7a mutations identified in our cohort represented as S26L, V82A, and T120I [20]. The emergence of these mutations is associated with the patient’s clinical manifestations, such as shortness of breath, considered one of the most severe COVID-19 symptoms. Furthermore, it may increase infectivity and reduce the immune response in vaccinated and unvaccinated individuals [20, 21].
The Delta and Omicron (the most common SARS-CoV-2 variant since early 2022) variants have several similar and different gene mutations. Computational studies established that the Omicron variant had a greater affinity to the human ACE2 receptor than the Delta variant due to the large number of mutations in SARS-CoV-2 RBD rendering it more transmissible (primarily due to mutations on the Q493R, N501Y, S371L, S373P, S375F, Q498R, and T478K). Additionally, the Omicron variant compared to the Delta variant contains a larger proportion of hydrophobic amino acids, like leucine and phenylalanine, across the whole S protein and the RBD [22]. Regarding the similarities, P681R is a mutation that both the Delta and Omicron variants shares [5] and facilitates the breakdown of the full-length S into S1 and S2, which might promote SARS-CoV-2 cell penetration [23].
This study has some limitations, particularly the small sample size as this study was conducted in the latter stage of the COVID-19 second wave when the cases started to decrease. In addition, patient outcomes (such as survival and long “COVID” phenomenon), viral load, and positivity duration were not investigated relative to their respective mutations. Nevertheless, the current findings provide valuable insights into the diversity and evolution of SARS-CoV-2 Delta variant mutations in the Indonesian population.
The predominant Delta SARS-CoV-2 variant sublineage in our cohort of Indonesian patients was AY.23 (69.39%), followed by AY.24, B.1.617.2 (original Delta variant), and AY.62. Furthermore, the S protein was the most frequently mutated region (12 mutations), with mutations also identified in the M protein, N protein, ORF, and NSP. Since new SARS-CoV-2 variants with increased transmissibility, immune evasion, and disease severity can result in a significant loss of human life, continuous genomic surveillance is required for early detection and implementation of public health interventions to contain future outbreaks.
COVID-19: coronavirus disease 2019
M: membrane
N: nucleocapsid
NSP: nonstructural protein
ORF: open reading frame
RBD: receptor-binding domain
S: spike
SARS-CoV-2: severe acute respiratory syndrome coronavirus 2
WHO: World Health Organization
PL: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data curation, Writing—original draft, Supervision. MAM: Software, Formal analysis, Investigation, Data curation, Writing—original draft. ER: Methodology, Formal analysis, Resources, Data curation, Supervision. RPP: Methodology, Resources, Data curation, Supervision. KYR: Methodology, Data curation, Writing—original draft, Supervision. NAS: Validation, Resources, Data curation. TPU: Software, Validation, Writing—review & editing, Visualization. All authors have read and approved the final version of the manuscript.
The authors declare that they have no conflicts of interest.
The Faculty of Medicine, Universitas Sriwijaya Ethics Review Committee granted ethical clearance for the investigation (approval number: 242-2022).
Informed consent was not needed due to the retrospective nature of this study; therefore, it was exempted by the Faculty of Medicine, Universitas Sriwijaya Ethics Review Committee.
Not applicable.
Data are available upon reasonable request from the corresponding author.
Not applicable.
© The Author(s) 2023.
Copyright: © The Author(s) 2023. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 5064
Download: 50
Times Cited: 0
Kamran Zaman ... Ranjit Sah
Wael Abu Ruqa ... Antonio Minni
Anna Antipov, Nikolai Petrovsky
Oliver Meek ... Miles W. Carroll
Hend Radwan ... Mohamed El-Kassas