Original Article
Original Article

Affiliation:
1Department of Clinical Psychology, School of Health in Social Science, The University of Edinburgh, EH8 9AG Edinburgh, UK
Email: c.calia@ed.ac.uk
ORCID: https://orcid.org/0000-0003-2505-6361
Affiliation:
2Department of Psychological Sciences and Health, University of Strathclyde, G1 1XQ Glasgow, UK
ORCID: https://orcid.org/0000-0002-2412-648X
Explor Med. 2024;5:401–415 DOI: https://doi.org/10.37349/emed.2024.00227
Received: January 25, 2024 Accepted: April 20, 2024 Published: June 06, 2024
Academic Editor: Hua Su, University of California, USA
The article belongs to the special issue Neurophysiological Mechanisms of Aging and Dementia
Aim: The present study investigated whether commonly used screening tools and assessments for dementia were culturally appropriate for older adults from ethnic minorities (EM) groups living in the UK.
Methods: Both South Asian and British participants (N = 43) were assessed using the Cross-Linguistic Naming Test, Mini Addenbrooke’s Cognitive Examination, Visual Short-Term Memory Binding Test (VSTMBT), and the Rowland Universal Dementia Assessment Scale. Multi-Ethnic Acculturation Scale and English proficiency, measured with a self-rated scale, were associated with the four respective. No interpreters were used.
Results: While members from EM significantly differed from members of the ethnic majority group in traditional neuropsychological tasks, their performance on the VSTMBT yielded results comparable to those drawn from the ethnic majority group. Complex influences seem to drive the sensitivity of traditional neuropsychological tasks to sociocultural factors.
Conclusions: This is the first study that subjects the VSTMBT to investigation in EM groups. Older adults from EM showed no impact of their sociocultural backgrounds on the function assessed by this test. However, other tests widely used for the assessment of EM populations proved sensitive to the investigated sociocultural factors. Our results lend support to the suggestion that neuropsychological assessments must abandon the one-size-fits-all notion when it comes to dementia risk detection among EM groups.
There are around 25,000 dementia patients with ethnic minority (EM) backgrounds in the United Kingdom, and this figure is anticipated to double by 2025 [1–4]. As a result, neuropsychologists will inevitably interact with individuals from diverse cultural, linguistic and educational backgrounds throughout their clinical practices [5]. Such a context poses challenges for health professionals and policymakers attempting to guarantee equity in health care [6]. Members of EMs are often diagnosed later than the rest of the population [7, 8] due to late (self)referrals and lack of appropriate tests and staff training [4, 9–11]. Therefore, it is increasingly important to develop instruments to screen for dementia in people from EM groups [12]. Although symptoms of dementia do not differ between different races and ethnicities, cross-cultural assessment of dementia can often be challenging for several reasons including: 1) lack of culturally valid tools for assessment, 2) language barrier, 3) culturally embedded stigma and taboo, 4) impact of stereotype threat (assumption by the examiner/cultural majority that people from a different cultural background will perform more poorly than people from a cultural majority background) and 5) prejudice on the part of the clinician or patient [11, 13]. One problem is the potential for misdiagnosis (false positive/negative) of cognitive decline amongst EM. The cognitive tests that are often used for cognitive screening are in many cases not suitable for people with a minority background (e.g., MMSE [14]). Linguistic, cultural, and educational factors have been shown to significantly influence cognitive test results [15–18]. Most available tests were developed in Western countries and have not gone through proper validation for their use in cross-cultural settings. They are therefore prone to cultural, educational, and linguistic biases [19, 20], rendering their use with EM groups inappropriate. Neuropsychological tests designed and standardized to measure constructs in one culture may not be readily applied to individuals of other cultures, with an expectation that they will equally measure the same construct [21–23]. This problem is exacerbated by a large gap in the literature for validation of neuropsychological tests for EMs in the UK [24]. There is a growing need of brief culture-free screening tool for dementia [25–30].
As briefly mentioned above, a strategy to overcome cultural bias is the development of theory-driven cross-cultural neuropsychological tests [31, 32] that possess properties of dementia markers [33]. Such tests would avoid the use of culture-specific or verbal stimuli [34]. Culture-free or unbiased tests could be used in the same format in different cultural contexts, removing the need for lengthy and laborious adaptations that often undermine their construct validity. By minimising linguistic elements, they have the potential to be suitable for individuals from EMs being assessed in a language other than their own [12, 35]. An example is the Rowland Universal Dementia Assessment Scale (RUDAS [36, 37]), a screening test developed as an alternative to the MMSE to minimize the effects of culture, language, and education on assessment outcomes [38].
An important challenge cross-cultural neuropsychology faces in global societies is linked to health service providers [10, 11]. Fujii [10] highlighted the challenge that assigning non-native English speakers with the assistance of translators poses to neuropsychologists. When investigating cognitive function in individuals with a minority background, where language constitutes a barrier, it is recommended to use a professionally trained interpreter who speaks the person’s mother tongue [13, 39]. Healthcare professionals often lack training in working with interpreters which could lead to poor communication, and, in turn, affect the quality of clinical evaluations [40, 41]. Using non-professional interpreters can result in inaccuracy in assessment outcomes, loss of confidentiality, and conflicts of interest [42]. A skilled interpreter can help prevent misdiagnosis when tests are administered in a non-native language [43, 44]. However, brief cognitive screening tools are often administered by practitioners in primary care settings where interpreters may be unavailable [45, 46]. Worldwide there are around 6,800 different languages, interpreters for each language are simply unrealistic [47]. Furthermore, using interpreters does not reduce the impact of culturally inappropriate content on test performance [48]. Taken together, the paucity of professional interpreters available in health settings across the world [11, 13], the risk of literal translation masking clinically relevant details [49], and the possibility of translator biases, i.e., answer on the patients’ behalf [50], render the use of interpreters an unreliable source.
The current study aimed to investigate whether four cognitive tests used to screen for dementia, namely the Mini Addenbrooke’s Cognitive Examination (M-ACE [51]), Cross-Linguistic Naming Test (CLNT [52]), the Rowland Universal Dementia Assessment Scale (RUDAS [34]), the Visual Short-Term Memory Binding Test (VSTMBT [53, 54]), reveal any bias in performance associated to participants’ ethnicity. Additionally, the effects of education, acculturation and language proficiency, as potential drivers of performance bias, were also investigated [55], along with self-rated English proficiency scores. A key methodological characteristic of the study is that we did not use interpreters. We predicted that, since a limited language involvement is required for the VSTMBT, performance on this test would be insensitive to the ethnic background of those assessed, a pattern that would not hold for the other screening tests.
To be eligible, participants had to be aged 60 or over, resident in the UK and needed to meet the following group-specific criteria:
1. EM group: a) identify as belonging to a South Asian EM group, b) speak English as an additional (non-native) language, c) have sufficient mastery of English to understand test instructions and give informed consent. 2. Ethnic majority group: a) identify as belonging to the UK ethnic majority group, b) speak English as a first language. Participants were excluded if they met any of the following criteria: Diagnosis of dementia or any other neurological or health conditions (e.g., stroke, psychiatric illness) that may affect cognitive functioning; disabilities that could interfere with testing or would require special accommodations (e.g., uncorrected vision or hearing problems). No subjects who met the inclusion criteria were excluded due to the above criteria.
To determine whether participants included in each group were cognitively healthy, authors employed a combination of self-report and established inclusion/exclusion criteria. Self-report: Participants were asked to self-report their medical history, current health status, and any cognitive concerns at the start of the assessment. They were asked questions related to memory, attention, language abilities, and overall cognitive functioning. Self-report allows researchers to gather initial information about participants’ cognitive health directly from the individuals themselves.
The final sample consisted of 43 subjects. The EM group comprises South Asian participants (N = 23; but see footnote of Table 1 for missing data), mainly from India and Pakistan, as they represent the largest EM in Scotland at 2.7% of the total population [56] and 2.3% in the UK [57]. Ethnic majority participants (N = 20) were recruited through a combination of convenience, snowball, and purposive sampling.
CLNT was used to determine language proficiency. The CLNT is a short test that assesses a person’s ability to identify and name 40 English words included within six semantic categories: animals, actions, parts of the body, natural phenomena, external objects, and colours [52]. Items are based on the Swadesh word list, used in nearly all of the extant languages spoken today [52, 58, 59]. The 100 vocabulary words within the Swadesh list are designed to be entirely disparate within language families irrespective of their cultural, geographic, or environmental proximity [58, 59]. The test incorporates words within the Swadesh list to avoid the potential confound of tester unfamiliarity with a particular word due to a potential difference in linguistic background. For this reason, the Swadesh words are incorporated as they are considered to be more frequently used in nearly all of the extant languages spoken today [52]. Studies have also shown the CLNT to be culturally and linguistically sensitive amongst differing cultural groups from Columbia, Morocco, Spain [60] and Lebanon [61].
The M-ACE is the abbreviated version of the ACE-III [51], a screening test for dementia. The ACE-III is a widely adopted and validated test currently used in memory clinics and dementia research around the world. Cultural adaptations for various items have been made to the ACE-III when it has been translated into languages other than English [62]. Since the M-ACE places heavy emphasis on verbally mediated and language items [51], it is likely that the EM group using English as an additional language will underperform compared to the ethnic and linguistic majority group. M-ACE has also been shown to be culturally valid in Malaysian [63], Thai [64], and Chinese [65] populations. However, each of these studies examined translated versions of the M-ACE. To date, no study has indicated whether the English M-ACE is culturally appropriate and sensitive to immigrants and EM living within English speaking countries.
The RUDAS is a brief cognitive screening instrument for dementia. It was developed for ethnically diverse populations [36] and is less influenced by educational and cultural factors than the MMSE [20, 37, 66, 67]. The RUDAS has been translated into over 30 languages [68] with strong ecological validity [20], and it has been shown to have comparable diagnostic accuracy for dementia to other conventional dementia screening tools, such as the MMSE and the ACE-III [37, 66, 69].
It comprises of 6 subtests [36] with limited emphasis on linguistic abilities. Moreover, there is limited evidence on the acceptability of the RUDAS for non-native English speakers without support from interpreters. The RUDAS was originally developed for use with an interpreter if the clinician does not speak the first language of the patient [36]. In a systematic review of the RUDAS, all eleven studies used formal interpreters [20]. It is critical to determine whether the RUDAS is appropriate in situations where interpreters are unavailable. In a study by Gonçalves et al. [70], performance of participants with English as a first and second language was compared on the RUDAS, without an interpreter. Both groups performed similarly, indicating that the RUDAS can be administered in a participant’s second language. However, level of language proficiency was not measured, so all participants may have been highly proficient in English. Furthermore, while the validity of it has been established in a range of Western European countries [71] it is yet to be administered with a UK-based sample.
The VSTMBT is a theory-driven domain-specific cognitive assessment. It assesses the precise function of temporarily binding the features of complex objects (i.e., shape and colour) together. This function is different (i.e., dissociable) from the one needed to process either feature separately. Contrary to process-impure cognitive abilities or composite scores, the latter known to encapsulate several outcome measures without underpinning psychometric frameworks [72, 73], theory-driven domain-specific cognitive assessments stand a better chance of both detecting the disease earlier and with better specificity and advancing theories of memory decline in ageing and dementia [74]. Such psychometric properties explain why VSTMB is insensitive to normal ageing [i.e., independent of the hippocampus [75–77], which shrinks with age, and reliant on regions of the medial temporal lobe (MTL) known to remain intact across the lifespan—perirhinal/entorhinal cortex [78]]. However, such MTL regions (anterior MTL network) are known to be affected by Alzheimer’s disease much earlier than the hippocampus [79, 80]. This explains why the VSTMBT detects Alzheimer’s disease preclinically in its familial [54] and sporadic variants [27] even when other traditional neuropsychological tests fail to detect impairments. Logie et al. [33] suggested that a good marker for Alzheimer’s disease should be insensitive to normal ageing, sensitive and specific to Alzheimer’s disease, and insensitive to the education level, literacy and cultural background of those assessed. We have now contributed consistent evidence supporting the former two. This study aims to contribute new evidence suggesting that this new assessment also meets the third criterion above.
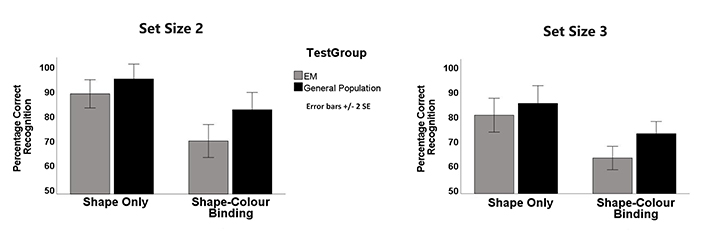
The VSTMBT has been considered a cross-cultural marker for Alzheimer’s disease [32]. During the VSTMBT, participants were presented with arrays of two or three abstract shapes displayed in random positions of a “3 × 3” virtual grid. After an initial fixation cross (1,000 ms), a study display was presented for 2,000 ms followed by a 900 ms unfilled retention interval. The test display was then presented and remained on until participants responded. Participants were asked to detect whether a change occurred between the study and the test display or if the stimuli remained the same. The task consisted of two conditions, the Single Shape condition assessed VSTMBT for single features. The Binding condition assessed VSTMBT for shape-colour bindings. During the Single Shape condition, participants were presented with either two or three black shapes, and in the Binding condition, two or three shapes were presented each in a different colour. To be able to detect such changes, participants had to remember either the individual shapes or the combinations of shape and colour (i.e., Binding condition) presented in the study display. Each condition consisted of 32 trials, of which 50% presented arrays of two stimuli and the remaining 50% presented three stimuli. The rationale for the use of these two set sizes was presented by Parra et al. (2019) [81]. We recorded the percentage of correct recognition per task condition and set size. The VSTMBT has been considered a cross-cultural marker for Alzheimer’s disease [32]. The function assessed by this test (i.e., binding in short-term memory), has proved insensitive to participants’ education and cultural background [82, 83].
Education—RQF is a score between 1–8 based on the UK’s Regulated Qualifications Framework (2019). Education Level was calculated by dividing three levels RQF [level 1 ≤ GCSE (General Certificate of Secondary Education); level 2 > GCSE; level 3 is a bachelor’s degree or higher]. Years in the UK, the percentage years in the UK and English proficiency were retrieved from the Multi-Ethnic Acculturation Scale (MAS [55]). English proficiency was recorded by a self-reported scale between excellent and poor from the MAS [55], the only acculturation scale designed for use with individuals from diverse ethnic groups [84]. This scale uses simple, commonly used vocabulary, suitable for linguistic minorities.
Data from neuropsychological tests were compared across groups using either independent-samples t-tests or Mann-Whitney U-tests (see Table S1 for normality checks and Table S2 for non-parametric tests). We reported on the outcomes from parametric tests here and those of non-parametric analysis are shown in Supplementary material. This methodological decision aims to demonstrate that the significance of the results observed was independent of the type of statistical analysis used. Variables from the VSTMBT were compared using a parametric 3-way mixed ANOVA model with Group (EM vs. ethnic majority) as the between-subjects factors, and Condition (shape vs. binding) and Set Size (2 vs. 3) as the within-subjects factors. A Group × Condition interaction will suggest potential cultural bias and this would be followed up with appropriate tests. If proved valid, we calculated the Binding Cost [7] which is the variable considered a marker for Alzheimer’s disease [27, 53, 54]. Finally, stepwise regression models were developed to explore underpinnings of the sensitivity of the screening tests investigated to sociocultural factors. The data were analysed using IBM SPSS Statistics (version 28).
The data collected in this manuscript were obtained in compliance with the Declaration of Helsinki. The study received ethical approval by the University of Edinburgh’s School of Health in Social Science (CLIN623). Every participant provided written consent. The average assessment time was approximately forty minutes.
There were some missing data in the final dataset [no significant differences in age, education, or gender were identified between groups (Table 1)]. However, statistical differences for years in the UK [t (34.99) = –7.60, P < 0.001], and percentages of years in the UK [t (28.95) = –8.84, P < 0.001], and English proficiency [t (40.24) = –6.50, P < 0.001] and MAS UK [t (41.00) = –5.21, P < 0.001] confirmed the appropriateness of the sample recruited to test the hypotheses here investigated.
There was a significant effect of Group [F (1,40) = 6.12, P = 0.018, η2 = 0.133]. Both the effect of Condition [F (1,40) = 66.89, P < 0.001, η2 = 0.63] and Set Size [F (1,40) = 33.31, P < 0.001, η2 = 0.45] were significant. Interestingly, none of the interactions reached the significance threshold [Group × Condition: F (1,40) = 2.43, P = 0.127, η2 = 0.06; Group × Set Size: F (1,40) = 0.41, P = 0.524, η2 = 0.01; Set Size × Condition: F (1,40) = 0.06, P = 0.805, η2 = 0.002; Group × Condition × Set Size: F (1,40) = 0.62, P = 0.805, η2 = 0.002] (Figure 1). We, therefore, collapsed performance across Set Size, and used such scores to calculate the Binding Cost [Binding Cost = (Performance on Shape-Only – Performance on Shape-Colour Binding)/Performance on Shape-Only * 100, [85]] which entered further analyses.
Among the neuropsychological tests, the CLNT [t (20.27) = –2.19, P = 0.04], M-ACE [t (29.52) = –3.42, P < 0.001] and RUDAS [t (27.82) = –2.16, P = 0.04] revealed significant differences across Group, while the VSTMBT, particularly the cost of binding [t (40) = 1.16, P = 0.27], did not (Table 1).
Demographic and cognitive characteristic
| Dependent Variables | Ethnic Minorities Group | Ethnic Minorities | Statistic | |||||
|---|---|---|---|---|---|---|---|---|
| N | Mean (SD) | N | Mean (SD) | t | df | P-value | CI 95% | |
| Age | 20 | 67.55 (6.19) | 22 | 66.59 (8.71) | –0.41 | 40.00 | 0.69 | (–5.71 3.80) |
| Education RQF | 20 | 8.05 (13.26) | 22 | 16.79 (20.89) | 1.63 | 35.94 | 0.11 | (–2.12 19.59) |
| Education level | 20 | 2.30 (0.57) | 22 | 2.50 (0.80) | 0.92 | 40.00 | 0.36 | (–0.24 0.64) |
| Years in the UK | 20 | 65.70 (7.71) | 23 | 39.84 (14.07) | –7.60 | 34.99 | < 0.001 | (–32.77 –18.95) |
| Percentage years in the UK | 20 | 97.37 (7.94) | 22 | 58.88 (18.63) | –8.84 | 28.95 | < 0.001 | (–47.38 –29.58) |
| English proficiency | 20 | 4.75 (0.55) | 23 | 3.48 (0.73) | –6.50 | 40.24 | < 0.001 | (–1.67 –0.88) |
| Multi-ethnic Acculturation Scale | 20 | 85.05 (12.10) | 23 | 64.61 (13.43) | –5.21 | 41.00 | < 0.001 | (–28.36 –12.52) |
| Neuropsychological tests | ||||||||
| Cross-Linguistic Naming Test | 20 | 39.90 (0.31) | 21 | 38.05 (3.87) | –2.19 | 20.27 | 0.04 | (–3.62 –0.09) |
| M-ACE | 20 | 27.15 (2.94) | 23 | 21.39 (7.44) | –3.42 | 29.52 | < 0.001* | (–9.20 –2.32) |
| RUDAS | 20 | 28.30 (2.64) | 22 | 24.95 (6.73) | –2.16 | 27.82 | 0.04* | (–6.52 –0.17) |
| VSTMBT Perception | 20 | 9.90 (0.31) | 22 | 9.64 (1.14) | –1.05 | 24.35 | 0.31* | (–0.78 0.26) |
| VSTMBT 2 Shapes | 20 | 15.10 (1.83) | 22 | 14.18 (2.22) | –1.45 | 40.00 | 0.15* | (–2.19 0.36) |
| VSTMBT 2 Bindings | 20 | 13.20 (2.19) | 22 | 11.27 (2.55) | –2.62 | 40.00 | 0.01* | (–3.42 –0.44) |
| VSTMBT Cost 2 | 20 | 12.54 (10.12) | 22 | 19.72 (16.39) | 1.73 | 40.00 | 0.09* | (–1.25 15.63) |
| VSTMBT 3 Shapes | 20 | 13.65 (2.43) | 22 | 12.91 (2.52) | –0.97 | 40.00 | 0.34* | (–2.29 0.81) |
| VSTMBT 3 Bindings | 20 | 11.75 (1.89) | 22 | 10.23 (1.54) | –2.87 | 40.00 | 0.01* | (–2.59 –0.45) |
| VSTMBT Cost 3 | 20 | 9.67 (30.68) | 22 | 18.4 (16.59) | 1.16 | 40.00 | 0.27* | (–6.45 23.90) |
M-ACE: Mini Addenbrooke’s Cognitive Examination; RQF: Regulated Qualifications Framework; RUDAS: Rowland Universal Dementia Assessment Scale; VSTMBT: Visual Short-Term Memory Binding Test. * not all the neuropsychological variables were normally distributed, see Tables S1 and S2, for non-parametric Mann-Whitney U tests. There were a few missing data from the Ethnic Minorities Group: one participant did not report on age or percentage years in the UK, and one did not report on education. One did not contribute data on the Cross-Linguistic Naming Test or RUDAS, and one did not contribute data on the Cross-Linguistic Naming Test or the VSTMBT
To explore the potential underpinnings of the sociocultural sensitivity shown by the neuropsychological screening tests, we ran regression models (Table 2). For the stepwise regression analysis, Group was first included as the predictor of interest (Model 1). A subsequent model included education level, years in the UK, percentage years in the UK, English proficiency, and the MAS as additional regressors (Model 2). Such an approach allowed assessment of whether variability on the cognitive screening tests could be accounted for by the participants’ ethnic background before (Model 1), and after (Model 2) controlling for sociocultural factors.
Regression model
| Dependent Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| R2 | ANOVA | Adj-R2 | ANOVA | |
| CLNT | 10.5% | F (1,39) = 4.56, P = 0.039 | 54.2% | F (3,35) = 15.98, P < 0.001 (a, d, f) |
| M-ACE | 20.4% | F (1,41) = 10.52, P = 0.002 | 22.2% | F (1,39) = 12.39, P = 0.001 (f) |
| RUDAS | 9.8% | F (1,40) = 4.33, P = 0.044 | 31.8% | F (2,37) = 10.08, P < 0.001 (c and d) |
| VSTMB Cost Total | 6.3% | F (1,40) = 3.76, P = 0.059 | No variables entered a model | |
ACE: Addenbrooke’s Cognitive Examination; CLNT: Cross-Linguistic Naming Test; RUDAS: Rowland Universal Dementia Assessment Scale; VSTMB Cost Total: Average of Visual Short-Term Memory Binding Cost 2 and 3. (a) Group, (b) education level, (c) years in the UK, (d) percentage years in the UK, (e) English proficiency, and the (f) MAS as additional regressors
Ethnicity was a significant predictor of CLNT. This predictive value remained significant after controlling for other sociocultural factors, with percentage of years in the UK and scores on the MAS also retained as significant predictors. Ethnicity significantly predicted performance on the M-ACE and RUDAS. However, after controlling for other sociocultural factors, ethnicity was no longer a significant predictor. The MAS was retained as a predictor of performance on the M-ACE whereas education level, years in the UK, and percentage of years in the UK were retained as predictors of performance on the RUDAS. Neither ethnicity nor other sociocultural factors yielded models that significantly predicted the cost of binding (see Table 2).
The presented study aimed to investigate whether cognitive tests used to screen for dementia revealed bias in test performance based on an individual’s ethnicity. The key points are: (1) Traditional neuropsychological tasks (CLNT, M-ACE and RUDAS) have proved sensitive to sociocultural variables whereas; (2) the VSTMBT proved insensitive. (3) Complex influences seem to drive the sensitivity of traditional neuropsychological tasks to sociocultural as demonstrated by regression models. We proceed to discuss these findings in turn.
Performance on the CLNT seems to be influenced by the percentage of years in the UK. The words found within the CLNT are derived from the Swadesh word list [58], a set of words considered to be universally found in most of the spoken languages. However, major criticisms have arisen about the degree to which the Swadesh words are universal [86]. The principal critique is that the Swadesh word list presumes that there are direct word equivalents between English and the many incorporated languages in the list. For example, the English word “you”, found in the Swadesh vocabulary, does not have a direct one-to-one word equivalent in other languages such as Urdu, a primarily South Asian language spoken by many throughout India and Pakistan [87].
Level of acculturation was a significant predictor of the M-ACE. The significant moderate correlation between acculturation and M-ACE suggests that higher adoption of the dominant culture is related to better test performance above age and education [84]. As culture represents adaptation to live in a specific context [88], what is relevant and worth learning for one individual in a particular cultural context may be less relevant for someone from another cultural background [89].
The M-ACE has been validated in different translated language versions [63–65], but it was not designed as a cross-cultural dementia assessment [51]. Thus, the results for the M-ACE test between the two cultural groups are not particularly surprising. These findings indicate that using the M-ACE in an EM group when administered in English may increase the risk in some ethnic groups performing below clinical cut-off scores, resulting in false diagnoses of cognitive deficit [90].
RUDAS seems affected by percentage of years in the UK and English proficiency. These results do not replicate the findings reported in the literature [34, 36, 67, 70, 71, 91, 92] which indicated that RUDAS scores were not significantly affected by culturally and linguistically diverse status. This discrepancy between the current and earlier studies may be explained by the use of interpreters in earlier studies [20, 37]. Cognitive scores on the RUDAS between the South Asian and British groups differed from previous studies [71]. The RUDAS was originally designed as a cross-cultural assessment for dementia and scores for both groups were expected to be similar [36]. One potential drawback of the RUDAS is the number of action tasks requiring constant feedback from both the tester and subjects (Praxis and Body Orientation Task) [36]. In fact, whereas CLNT and Mini-ACE only had one significant predictor of group differences, RUDAS had three (i.e., percentage of years in the UK, English proficiency and education level).
The VSTMBT has proved to be insensitive to the individual’s ethnicity. The VSTMBT indexes low level of visual functions and makes it language-independent, hence a high level of English proficiency is not required [32, 83]. The task relies on a simple set of instructions easy to understand and follow by people with little formal education and assessed in a language they are not proficient [33, 83]. It is also not affected by prior knowledge, experience, or nor practice effects. Previous studies showed that level of education does not affect the performance which indicates that it may be appropriate to test patients from various educational and socio-cultural backgrounds [32, 54], however, none of these earlier studies considered EMs. Here we have further demonstrated that even the most taxing version of this task (i.e., Set Size 3 [83]) did not render it more challenging for EMs. This is important because it was recently suggested that while the version with three items can aid dementia’s risk screening in asymptomatic stages, the version with two items would help detect Alzheimer’s disease dementia in its mild stage [83]. Our results suggest that EMs in the UK can benefit from such an assessment from the asymptomatic stages to the early clinical stages of the disease.
Our results suggest that a one-size-fits-all approach would not help identify the vulnerabilities of cognitive and neuropsychological assessment to sociocultural factors. Mungas et al. (2009) [93] suggested that such task properties would not only influence our interpretation of the association between sociocultural factors and behaviours, but also our interpretation of the association between brain pathology and behavioural outcomes. Complex influences seem to drive the sensitivity of traditional neuropsychological tasks to sociocultural as demonstrated by regression models. Different tests showed different vulnerabilities to different sociocultural factors, an observation that is in line with [93]. Taken together these results suggest that assessments for dementia risk in EM groups ought to consider a wide range of meaningful sociocultural factors when it comes to the selection of appropriate tools. For example, linguistic barriers significantly influence the accuracy and validity of the cognitive evaluation, despite the presence of a professional interpreter [94]. Our study is innovative because we investigated the effect of ethnicity on neuropsychological test results when administered in a language other than the participant’s native language without the use of interpreters. This allowed us to observe what can happen in the real clinical testing setting where interpreters are neither always available nor reliable [4, 12, 13].
Our study had some limitations. The small sample size may have led to some bias [95] considering that South Asians in the UK are not a homogeneous ethnic group, but include Indians 2.3%, Pakistanis 1.9%, Bangladeshis 0.7% and other Asians [57]. Although the South Asians and British were matched for age, education and gender; occupations between the two groups were not perfectly equivalent. In terms of predictor variables, English proficiency was a self-rated measure of language competence. As such, this proxy variable may not necessarily be reflective of the participants’ true level of English literacy in which self-knowledge bias may play a role [96]. EM differ from the majority group more than language. A range of variables are likely to contribute to the difference in test performance, such as acculturation [85], education [97] or socio-economic status [98]. The contributions of the latter variable cannot be fully disentangled by the present study because it was not collected for ethical reasons. Education was measured based on stratification of years of education. However, it is unlikely that quantitative variations in education reflect qualitative differences in education across countries with different education systems [99].
CLNT: Cross-Linguistic Naming Test
EM: ethnic minorities
M-ACE: Mini Addenbrooke’s Cognitive Examination
MAS: Multi-Ethnic Acculturation Scale
MTL: medial temporal lobe
RUDAS: Rowland Universal Dementia Assessment Scale
VSTMBT: Visual Short-Term Memory Binding Test
The supplementary tables for this article are available at: https://www.explorationpub.com/uploads/Article/file/1001227_sup_1.pdf.
Special thanks to Alfredo Ardila who provided both the Cross-Linguistic Naming Test and Multi-Ethnic Acculturation Scale.
CC: Conceptualization, Methodology, Investigation, Supervision, Writing—original draft, Writing—review & editing. MAP: Formal analysis, Writing—review & editing. Both authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
The data collected in this manuscript were obtained in compliance with the Declaration of Helsinki. The study received ethical approval by the University of Edinburgh’s School of Health in Social Science (CLIN623).
The informed consent to participate in the study was obtained from all participants.
Not applicable.
Datasets are available on request: The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
Not applicable.
© The Author(s) 2024.
Copyright: © The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Yixuan Wang ... Wei Qiao Qiu
P.V.N.N. Ranasinghe, Mapa S. T. Mapa
Daniel V. Guebel
Ahmed A. Gaballa ... Ahmed El-adawy
Anna Fabbrocino ... Fabrizio Vecchio