 Original Article
Original Article

Affiliation:
1Department of Surgical Sciences (DISC), Division of Prosthetic Dentistry, University of Genoa, 16132 Genoa, Italy
ORCID: https://orcid.org/0000-0002-5408-3345
Affiliation:
2Department of Biomedical Sciences, Humanitas University, 20089 Milan, Italy
Affiliation:
3Department of Mechanical Engineering, Polytechnic School, University of Genoa, 10129 Genoa, Italy
ORCID: https://orcid.org/0000-0002-6097-3184
Affiliation:
2Department of Biomedical Sciences, Humanitas University, 20089 Milan, Italy
Affiliation:
4Solid and Fluid Biomechanics Group, PolitoBIOMed Lab, Department of Mechanical and Aerospace Engineering, Turin Polytechnic School, 10127 Turin, Italy
ORCID: https://orcid.org/0000-0002-9660-5551
Affiliation:
5Department of Surgical Science, CIR Dental School, University of Turin, 10127 Turin, Italy
ORCID: https://orcid.org/0000-0003-1271-3334
Affiliation:
1Department of Surgical Sciences (DISC), Division of Prosthetic Dentistry, University of Genoa, 16132 Genoa, Italy
Email: jacopocolo@tiscali.it
ORCID: https://orcid.org/0000-0002-7206-6848
Explor Med. 2024;5:467–476 DOI: https://doi.org/10.37349/emed.2024.00232
Received: March 20, 2024 Accepted: May 07, 2024 Published: July 05, 2024
Academic Editor: Gaetano Isola, University of Catania, Italy
The article belongs to the special issue Biomaterials and Biomarkers in Dentistry: Up to Date
 A Correction to this article was published on 10 July 2024
A Correction to this article was published on 10 July 2024
Aim: Magnetodynamic surgery has assumed increasing importance in recent years. The purpose of the present study was to compare in vitro, using dry porcine ribs, two methods of dental implant site preparation (conventional drill and magnetic mallet) on three aspects of the site. These were the difference between the diameter of the site and the diameter of the last drill used (an index of the accuracy of the preparation), the weight loss of the specimen on which the site was prepared (index of the bone loss in the site), and the change of temperature at the site (an index of the change to the material at the site).
Methods: Eight preformed pork ribs were chosen for the study. Four implant preparations were made on each rib, two with Magnetic Mallet (Meta Ergonomica, Turbigo, Italy) and two with traditional drills. Each bone sample was weighed before and after implant site preparation in order to calculate the amount of bone lost during preparation. The diameter of preparations was analyzed with the aid of an optical microscope (MZ6, Leica, Wetzlar, Germany) connected to a dedicated measurement software. For the evaluation of the temperature, eight preparation sites were marked. In correspondence of each preparation site, on the opposite side of the rib, a hole was made for the thermocouple (HI 91530K, Hanna Instruments, Padova, Italy). During the preparations, the thermocouple was kept inserted inside the control hole to record the temperature variation. The results were analyzed using appropriate statistical methods, such as the Kolmogorov-Smirnoff test and the Wilcoxon test.
Results: It was found that mallet drill provided significantly higher accuracy of preparation, lower amount of damage at the site, and less change to the porcine rib test material at the preparation site.
Conclusions: A possible clinical implication of this finding is discussed.
The increasingly widespread use of dental implants and the need for less traumatic techniques has favored the development of ever more performing and less invasive instruments for the patient for the preparation of the implant bone site [1–5].
In particular, alternative technologies to the classic use of the drill have been proposed and studied since early 2000’s such as, for example, piezoelectric instrumentation [6, 7], and in recent years osseodensification drills and magnetodynamics [8–11], in order to reduce the inflammatory response and amplify the biomolecular factors involved in healing bone and in osseointegration [12].
Magneto-dynamic technology applies physical principles of electromagnetism to give controlled forces on a body minimizing the impact time. The control and steadiness of the applied forces make the procedures safe for patients and surgeons. Furthermore, the magnetodynamic technology working through the principle of osteocondensation allows a more conservative approach towards the tissues. Bone loss is probably more limited compared to the use of drills and the primary stability of the implant has been demonstrated by Stacchi et al. [8] to be comparable to that obtained with a preparation with drills. Other authors such as Negidah et al. [13] even maintain that in vivo the results in terms of implant stability quotient (ISQ) are better than with drills. Despite this study has a major shortcoming given by the small number of the sample analyzed.
Magnetic mallet is composed of a handpiece energized by a power control device, delivering forces by the timing of application. Different inserts could be attached to the handpiece. Mallet can be set on four forces: 75, 90, 130, and 260 daN. Impact time is 80 μs.
Magnetodynamic instrumentation, applied to bone surgery, has given new impetus in recent years and the first results of use seem to be encouraging, in particular as regards the preparation of the implant site [14–16].
As shown by Bennardo et al. [17] in a recent review, magnetodynamic could be helpful in implant surgery, in terms of tissue healing, surgery outcome, and complication rate compared to traditional instruments. However, some aspects of the use of magnetodynamics for the preparation of the implant site require further investigation, also in relation to the comparison with the instruments of choice, i.e., the drills.
An extremely important aspect is that of bone overheating during the site preparation phases, the evaluation of the temperature increase is a fundamental aspect that influences post-operative bone healing [18–22]. Heat production as demonstrated by Bhargava et al. [23] turns out to be essentially zero in the use of manual osteotomes. This has yet to be demonstrated in use with magnetodynamic technology.
The purpose of the present study was to compare two methods of dental implant site preparation (conventional drill and magnetic mallet) on three aspects of the site. These were the difference between the diameter of the site and the diameter of the last drill used (an index of the accuracy of the preparation), the weight loss of the porcine rib specimen on which the site was prepared (index of the extent of damage at the site caused by the preparation), and the change of temperature at the site (an index of the change to the porcine rib specimen at the site).
The null hypothesis is that drills and magnetodynamic instruments have the same behavior.
Eight preformed pork ribs all of similar size and thickness were obtained from Tecnoss® Dental s.r.l. (Turin, Italy), a commercial company that provides bone materials for education. The accuracy of the implant site preparations and change in weight before and after preparations was analyzed. It has been used dry bone stored in vacuum, opened and used immediately. We did not consider environmental conditions in this study. It is an industrially prepared dry bone suine origin.
In particular, the ribs have a crestal width of about 5 mm and a cortical thickness of about 2 mm. The medullary bone has a consistency of the D3 of Misch’s classification. This type of rib was chosen for the possibility of having uniform cortical thickness and bone density.
The ribs are divided into a part already prepared with the removal of the cortical bone and an intact part. For this first phase of the study, it was decided to use the part without the cortex to better evaluate the bone expansion and the accuracy of the preparation hole.
The ribs were weighed before the preparations began in order to have the starting weight.
Four implant preparations were made on each rib, 2 with Magnetic mallet (Meta Ergonomica, Turbigo, Italy) using the plus handpiece and 2 with traditional burs, dedicated surgical motor (EXPERTsurg, KaVo, Biberach, Germany) and surgical handpiece (SURGmatic S201 XL, KaVo, Biberach, Germany). The positions of the preparations were numbered from A to D and the choice of which instrument to use was made randomly before starting according to Table 1. Randomization was obtained by drawing lots.
Distribution of the preparation tools in the analyzed samples
| Samples | Position A | Position B | Position C | Position D |
|---|---|---|---|---|
| Sample 1 | Mallet | Drill | Mallet | Drill |
| Sample 2 | Drill | Mallet | Drill | Mallet |
| Sample 3 | Mallet | Drill | Mallet | Drill |
| Sample 4 | Drill | Mallet | Drill | Mallet |
| Sample 5 | Mallet | Drill | Mallet | Drill |
| Sample 6 | Drill | Mallet | Drill | Mallet |
| Sample 7 | Mallet | Drill | Mallet | Drill |
| Sample 8 | Drill | Mallet | Drill | Mallet |
All preparations were made by an expert oral surgeon (surgeon: D.B.).
It was decided to perform preparations at a depth of 15 mm following the systematic for the insertion of conical implants (AnyRidge, MEGAGEN, Seoul, South Korea). Choosing a depth of 15 mm there is a perfect correspondence between the diameter of the last drill and that of the last mallet insert (BLK-R3), i.e., 3.3 mm. This guarantees adequate under-preparation for the insertion of a 3.8 mm in diameter.
For the preparation with drills, the method indicated by the manufacturer was followed and then passages of the drills in sequence with increasing diameters: lanceolate drill for the thickness of the cortex and then preparation drills brought to the working length with diameters of 2 mm, 2.5 mm, 2.8 mm and 3.3 mm.
The drills were all used with a speed of 1200 rpm/min with irrigation set to level 3 of 5 of the implant motor used (Figure 1A).
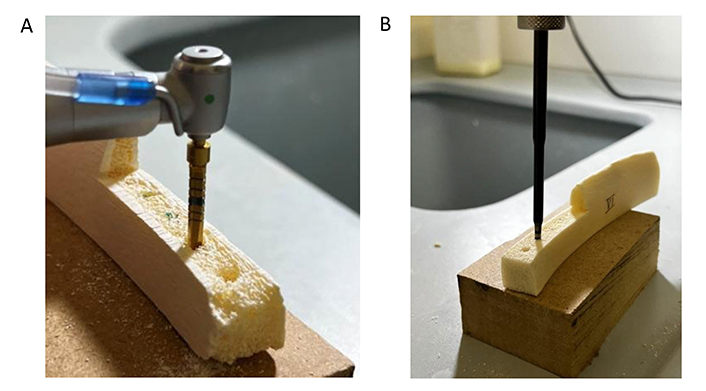
Preparation with drill (A) and mallet (B) on the part of the rib to be used for the study of the expansion (from top to bottom as position A, B, C, D)
For the preparation of the implant site with magnetic mallet it was decided to use the osteotomes of the Black Ruby series (Meta Ergonomica, Turbigo, Italy), specifically designed for the preparation of the implant site (Figure 1B).
The preparation sequence involved the use of osteotomes in increasing sequence up to the working size: FIRST, BLK-R1, BLK-R2, BLK-R3.
Each bone sample was weighed before and after implant site preparation in order to calculate the amount of bone lost during preparation and to rule out any weight gain due to cooling fluid. Measurements were obtained by a precision balance that provides centesimal precision with an error variance of ± 0.02 g (Gram EH 500, Waagenet AF GmbH, Berlin, Germany).
The preparations were analyzed with the aid of an optical microscope (MZ6, Leica, Wetzlar, Germany) connected to a dedicated measurement software (Leica Map Start, Leica, Wetzlar, Germany) (error variance ± 1 µm).
Using the software, the diameter of the preparation hole was measured for each preparation to verify the accuracy of the magnetic insert and the drill (Table 2).
Diameters in mm of the preparation holes
| Samples | Position A | Position B | Position C | Position D |
|---|---|---|---|---|
| Sample 1 | 3.53 Mallet | 3.87 Drill | 3.32 Mallet | 3.56 Drill |
| Sample 2 | 3.36 Drill | 3.23 Mallet | 3.37 Drill | 2.95 Mallet |
| Sample 3 | 3.20 Mallet | 3.45 Drill | 3.14 Mallet | 3.50 Drill |
| Sample 4 | 3.38 Drill | 3.36 Mallet | 3.45 Drill | 3.24 Mallet |
| Sample 5 | 3.35 Mallet | 3.49 Drill | 3.25 Mallet | 3.60 Drill |
| Sample 6 | 3.38 Drill | 3.23 Mallet | 3.50 Drill | 3.15 Mallet |
| Sample 7 | 3.04 Mallet | 3.41 Drill | 3.40 Mallet | 3.37 Drill |
| Sample 8 | 3.43 Drill | 3.31 Mallet | 3.43 Drill | 3.23 Mallet |
After each preparation, the ribs were weighed in order to be able to compare the amount of bone lost during preparation with the starting weight and to exclude any increase in weight due to the cooling liquid (Table 3).
Summary of the pre- and post-site preparation weights (in g) of the porcine rib specimens
| Samples | Position A pre | Position A post | Position B pre | Position B post | Position C pre | Position C post | Position D pre | Position D post |
|---|---|---|---|---|---|---|---|---|
| Sample 1 | 27.67 | 27.62 Mallet | 27.62 | 27.56 Drill | 27.56 | 27.52 Mallet | 27.52 | 27.44 Drill |
| Sample 2 | 29.44 | 29.40 Drill | 29.40 | 29.39 Mallet | 29.39 | 29.33 Drill | 29.33 | 29.30 Mallet |
| Sample 3 | 30.29 | 30.23 Mallet | 30.23 | 30.18 Drill | 30.18 | 30.17 Mallet | 30.17 | 30.10 Drill |
| Sample 4 | 32.48 | 32.44 Drill | 32.44 | 32.44 Mallet | 32.44 | 32.40 Drill | 32.40 | 32.40 Mallet |
| Sample 5 | 25.69 | 25.66 Mallet | 25.66 | 25.62 Drill | 25.62 | 25.61 Mallet | 26.61 | 26.59 Drill |
| Sample 6 | 24.64 | 24.61 Drill | 24.61 | 24.60 Mallet | 24.60 | 24.59 Drill | 24.59 | 24.57 Mallet |
| Sample 7 | 26.33 | 26.33 Mallet | 26.33 | 26.29 Drill | 26.29 | 26.29 Mallet | 26.29 | 26.25 Drill |
| Sample 8 | 28.78 | 28.75 Drill | 28.75 | 28.75 Mallet | 28.75 | 28.73 Drill | 28.73 | 28.72 Mallet |
The measurements obtained were subjected to statistical analysis.
For the second part of this study, the evaluation of the temperature, 5 ribs were chosen with the same characteristics as those used for the evaluation of bone expansion (Tecnoss® Dental s.r.l., Turin, Italy), using in this case the part of the ribs which also had the presence of the cortical bone (Figure 2).

Ribs used for the evaluation of temperature changes (from top to bottom as position A, B, C, D, E, F, H)
Eight preparation sites were marked on each rib with letters from A to H and the choice of the instrument to be used in each site was randomly decided before the study according to the scheme in Table 4, obtained by drawing lots.
Distribution of the preparation tools in the analyzed samples
| Samples | Position A | Position B | Position C | Position D | Position E | Position F | Position G | Position H |
|---|---|---|---|---|---|---|---|---|
| Sample 1 | Mallet | Drill | Mallet | Drill | Mallet | Drill | Mallet | Drill |
| Sample 2 | Drill | Mallet | Drill | Mallet | Drill | Mallet | Drill | Mallet |
| Sample 3 | Mallet | Drill | Drill | Mallet | Mallet | Drill | Drill | Mallet |
| Sample 4 | Drill | Mallet | Mallet | Drill | Drill | Mallet | Mallet | Drill |
| Sample 5 | Mallet | Drill | Mallet | Drill | Mallet | Drill | Mallet | Drill |
In correspondence with each preparation site, on the opposite side of the rib, a hole was made with a 1 mm diameter cutter for the thermocouple (HI91530K, Hanna Instruments, Padova, Italy) (error variance ± 0.1 °C) calculating its depth so as to arrive at 1 mm from the apex of the implant preparation (Figure 3) [15, 16].
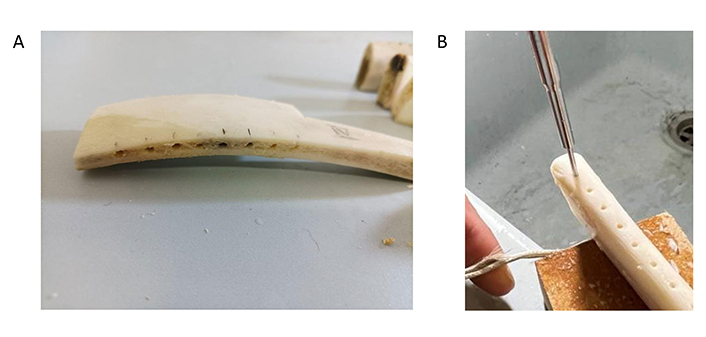
Thermocouple insertion and positioning. (A) Detail of the hole for inserting the thermocouple. (B) Position of the thermocouple during mallet preparation (from right to left as position A, B, C, D, E, F, H)
Eight preparations were made on each rib, 4 with drills and 4 with mallet.
All preparations were made by one expert surgeon (surgeon: D.B.).
For the preparation with drills, the method indicated by the manufacturer was followed and then passages of the drills in sequence with increasing diameters: lanceolate drill to pass the thickness of the cortex and then preparation drills taken to the working size with diameters 2 mm, 2.5 mm, 2.8 mm and 3.3 mm.
Drills were all used at a speed of 1200 rpm/min with irrigation set to level 3 of 5 of the implant motor used.
For the preparation of the implant site with magnetic mallet it was decided to use the osteotomes of the Black Ruby series (Meta Ergonomica, Turbigo, Italy), specifically designed for the preparation of the implant site.
The preparation sequence involved the use of a lanceolate bur to go beyond the thickness of the cortex and then the use up to the working size of the osteotomes in increasing sequence: FIRST, BLK-R1, BLK-R2, BLK-R3.
Both during the preparation with the drill and with the osteotomes, the thermocouple was kept inserted inside the control hole to record the temperature variation during the preparations. Control hole that has been isolated with film to prevent the coolant from altering the measurements (Figure 3B).
The data collected was then sent to statistics for the related analyses.
A statistical analysis was conducted in order to investigate the influence of two different tools (i.e., magnetic mallet and dental drill) on the obtained site diameter and the bone weight and temperature variation during the procedure.
The power of the adopted statistical test was evaluated through the following equation for the required sample size estimation for pairwise comparisons of two populations:
where
With a significance level
Nd = 14 for the obtained diameter
Nw = 18 for the weight variation
Nt = 15 for the temperature variation
Since the number of samples involved in the study was Nd = 16, Nw = 18, and Nt = 20, the power of each pairwise analysis is at least 80%.
The results were analyzed using MATLAB (MATLAB, MathWorks Inc., Natick, USA).
A statistical analysis was conducted in order to investigate the influence of two different tools (i.e., magnetic mallet and dental drill) on the obtained site diameter and the bone weight and temperature variation during the procedure.
The following figures show the mean and standard deviation of the aforementioned variables measured after surgery performed using magnetic mallet and the dental drill.
A Kolmogorov-Smirnov test was performed to investigate data normality, and since data were not normally distributed, non-parametric tests (i.e., statistical tests which do not assume any specific distribution for the data) were adopted for pairwise comparisons.
In this study, it has not been performed any kind of examination of the microscopical features at the preparation sites.
Summary of the results for change in diameter of the prepared site.
A two-sample Wilcoxon test highlighted significant differences between the diameter obtained with magnetic mallet and the dental drill (P < 0.01) (Figure 4A).
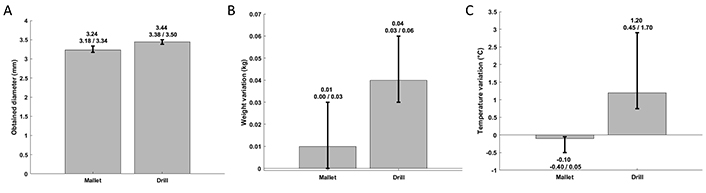
Summary of experimental outcomes. (A) Summary of preparation site diameters. (B) weight variation after intervention. (C) changes in temperature in the prepared site. Numbers indicating the mean, maximum, and minimum values for the experimental group above the bar chart
Summary of the results for change in weight of the porcine rib specimens.
A two-sample Wilcoxon test highlighted significant differences between the bone weight variation obtained with magnetic mallet and the dental drill (P < 0.01) (Figure 4B).
Summary of the results for change in temperature in the prepared site.
A two-sample Wilcoxon test highlighted significant differences between the bone temperature variation obtained with magnetic mallet and the dental drill (P < 0.01) (Figure 4C).
In the last ten years, the application of magnetodynamics to oral surgery has increased.
The first studies by the group of Crespi et al. evaluated the in vivo use of magnetodynamics applied to split crest, osteocondensation and sinus floor elevation techniques [9, 10, 11, 15, 16]. These studies are conducted on a good number of patients, but the main evaluation is based only on measurements on intraoral X-rays and the follow-up is short.
Negidah et al. [13] evaluated the ISQ on a patient, finding that the mallet offers better results than the drill. This study is interesting for in vivo application, but follow-up and sample size are extremely poor.
Bhargava et al. [23] evaluated heat production and changes in bone structure by comparing piezoelectric instruments, manual osteotomes, traditional drills and osteocondensers, finding that the osteotome offers results comparable to the drill in terms of heat development, but better in terms of bone preservation.
Schierano et al. [12] in in vivo studies on pigs they demonstrate by histologically and histomorphometrically analyzing the samples that preparing the implant site with a mallet improves healing compared to the drill.
A case report has highlighted good clinical possibilities regarding osteocondensation and increases in bone volume with the magnetodynamic technique [24].
In the literature, only one review conducted by Bennardo et al. [17] investigated the actual usefulness of this technique in implant insertion. The authors conclude that the technique can be useful but that it needs further studies to be validated.
The analysis of the accuracy of preparation (∆D), change of weight of the rib specimen (∆W), and change of temperature in the hole produced (∆T) aims to analyze three aspects on which the literature does not present data certain.
All three variables considered demonstrate a statistically significant difference between magnetodynamic instrument and drill.
In particular, the first variable analyzed was the accuracy of preparation (∆D). We know that the drill always creates a slight overpreparation with respect to its diameter [25]. The mallet has been shown to create a final preparation diameter that is more faithful to that created by the bur. Furthermore, the observation suggests that in very dense bone (cortical) there may be an important elastic return of the bone itself with respect to the moment in which the instrument is disengaged. This phenomenon could lead to an increase in primary stability in the case of implant placement.
The use of the magnetic mallet has the ability to modify, making some surgical techniques more predictable and effective. The variables of temperatures, accuracy of preparation and ability to preserve the tissues have allowed us to test the behavior of the mallet in situations where the use of a traditional technique can give us disadvantages.
Change of weight of the rib specimen (∆W) is statistically lower, this is explained by the fact that the mallet works by condensation of the bone tissue while the drill by removal. As suggested by Bhargava et al. [23], one advantage of the mallet is that with its use, there is an increase in primary stability, especially in low quality bone.
As postulated by Timon and Keady [22], the increase in temperatures above 50°C can cause bone necrosis and consequent problems for osseointegration. The mallet allows you to prepare the implant site without creating potential damage from overheating. However, both instruments do not come close to the temperature limit and can be considered safe.
Particular attention in the use of the mallet instrument must be placed in the presence of thick cortices or very high-quality bone. In these cases, the user must be careful to avoid triggering fracture lines within the affected cortical bone.
The results obtained in this study regarding the accuracy of the preparation (∆D) and change of weight of the rib specimen (∆W) are in line with what the literature has indicated until now. Although the osteocondensation capacity was mainly analyzed in vivo in an indirect manner by evaluating the implant stability. The change in weight provides us with a qualitative assessment of the loss of bone volume during preparations. These parameters are decisive in the clinical choice of surgical technique.
The main limitation of this study is using dry porcine ribs is quite far from clinical situation, despite using of cooling fluid, and it could modify heat development. It would be interesting to investigate temperature variations in fresh ribs.
The results obtained in this study validate the clinical use of the magnetodynamic technique. It is clear that the greater the precision of the preparation with respect to the implant body, the better the primary stability will be. The same thing can be applied to the concept of osteocondensation by analyzing through the weight of the samples. Especially in poor quality bone, the possibility of condensing it improves primary stability.
The temperature increase in the bone during preparation is clinically an important variable that can influence the success of the treatment. The mallet has been shown not to cause temperature increases, making it a safe instrument.
In conclusion, the main finding of the study was that for dental implant site preparation on an animal model (pig ribs), magnetic mallets provided significantly higher accuracy of preparation, lower amount of damage at the site, and smaller change of temperature at the site compared to when standard drills were used. These findings may provide guidance to clinicians in the choice of site preparation method.
DB: Conceptualization, Methodology, Investigation, Supervision, Project administration. JM: Conceptualization, Methodology, Investigation, Visualization, Supervision. EL: Resources, Data curation. CB: Investigation, Visualization. ATL: Data curation. GS: Writing—review & editing. JC: Methodology, Investigation, Writing—original draft, Writing—review & editing. All authors have read and agreed to the published version of the manuscript.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
The data for this study can be found by asking the corresponding author.
Not applicable.
© The Author(s) 2024.
Copyright: © The Author(s) 2024. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

Simona Santonocito ... Gaetano Isola
Saeed Asgary, Laleh Alim Marvasti
Elio Minetti ... Francesco Inchingolo
Renzo Guarnieri ... Luca Testarelli
Salwa Mekled ... Geraldine Weinstein
