Perspective
Perspective

Affiliation:
Department of Senior Exercise Prescription, Gwangju Health University, Gwangju 62287, Republic of Korea
Email: hjkim@ghu.ac.kr
ORCID: https://orcid.org/0000-0001-6538-3872
Explor Med. 2025;6:1001282 DOI: https://doi.org/10.37349/emed.2025.1001282
Received: November 26, 2024 Accepted: January 26, 2025 Published: February 18, 2025
Academic Editor: Marco Cascella, University of Salerno, Italy
The article belongs to the special issue Innovative Approaches to Chronic Pain Management: from Multidisciplinary Strategies to Artificial Intelligence Perspectives
Chronic pain, affecting approximately 30.3% of adults worldwide, presents a significant global health issue, severely impacting individuals’ quality of life and creating substantial socioeconomic challenges. Traditional pain management methods, such as physical therapy and pharmacological treatments, primarily focus on the biological aspects of pain while often neglecting the psychological and social factors. However, recent advancements in neuroscience have revealed that chronic pain is influenced by changes in the central nervous system, including mechanisms like central sensitization and neuroplasticity. This paper examines contemporary neuroscience-informed interventions, including Pain Neuroscience Education (PNE), mindfulness practices, and cognitive functional therapy (CFT), which target these neurobiological changes to improve pain perception and behaviors. These interventions help rewire the brain’s pain pathways, promoting long-term pain relief and functional recovery. Additionally, combining neuroscience-based approaches with conventional therapies has been shown to enhance treatment outcomes. This work emphasizes the need for personalized approaches and the integration of emerging technologies to enhance the accessibility and effectiveness of chronic pain management.
Chronic pain, defined as pain persisting for over three months, is a significant global health concern that impacts approximately 30.3% of adults worldwide [1]. Musculoskeletal chronic pain, in particular, not only diminishes individuals’ quality of life but also leads to substantial socioeconomic challenges, including increased healthcare expenditures and reduced workforce productivity [2]. The World Health Organization estimates that chronic pain results in an annual global economic loss of approximately $500 billion [3].
Traditional approaches in rehabilitation medicine for managing chronic pain have focused on strategies like physical therapy, exercise therapy, and pharmacological treatments [4]. While these methods primarily target the biological aspects of pain, they often overlook the psychological and social dimensions that contribute to the overall pain experience [5]. Recent advancements in neuroscience have demonstrated that chronic pain is a multifaceted condition, strongly linked to alterations in the central nervous system (CNS) [6, 7].
In light of these findings, neuroscience-informed interventions have gained increasing attention within the rehabilitation field [8]. Techniques such as Pain Neuroscience Education (PNE), mindfulness practices, and cognitive functional therapy (CFT) have shown effectiveness in reshaping pain perception and encouraging adaptive behaviors among individuals with chronic pain [9, 10]. These interventions utilize the principle of neuroplasticity to rewire pain-related neural pathways and manage central sensitization effectively [10–12].
This paper aims to explore the neuroscientific foundations and clinical applications of contemporary interventions in chronic pain management. It provides a systematic review of the neurobiological mechanisms, practical implementation protocols, and long-term efficacy of these methods, offering clinicians valuable insights for integrating these approaches into practice.
Understanding the neurobiological mechanisms of chronic pain forms the cornerstone for developing modern intervention strategies [13]. Recent advancements in neuroscience have revealed that chronic pain extends beyond peripheral tissue damage or inflammatory responses, involving complex changes within the CNS [14].
The concept of the pain neuromatrix explains that pain is not merely a sensory experience but the result of the activation of a multidimensional neural network [15]. This network includes interactions among various brain regions such as the somatosensory cortex, anterior cingulate cortex, and insula, integrating the sensory, emotional, and cognitive dimensions of pain [16].
Central sensitization, one of the key mechanisms of chronic pain, refers to increased CNS sensitivity in processing pain signals [7]. This phenomenon involves changes in synaptic plasticity, heightened activation of NMDA receptors, and impaired descending pain modulation systems [17]. Consequently, the pain threshold is lowered, leading to phenomena such as hyperalgesia (heightened pain sensitivity) and allodynia (pain from normally non-painful stimuli) [18].
Neuroplasticity is a critical concept for understanding the structural and functional changes in the brain associated with chronic pain [19]. Functional magnetic resonance imaging (fMRI) studies have documented cortical thickness alterations, decreased gray matter density, and rewiring of neural circuits in chronic pain patients [20]. Importantly, these changes are often reversible, highlighting the potential for recovery through therapeutic interventions [21].
Psychosocial factors influencing pain experiences also have distinct neurobiological underpinnings [22]. Emotional states such as stress, anxiety, and depression enhance pain sensitivity through activation of the hypothalamic-pituitary-adrenal (HPA) axis and may also impact immune system function [23]. Additionally, social support and environmental factors are known to modulate endogenous pain control systems [24–26].
The recognition of these psychosocial influences has led to the development of targeted interventions that specifically address these factors while acknowledging their neurobiological underpinnings. The following section explores how contemporary mind-body interventions effectively integrate this understanding into practical therapeutic approaches.
Contemporary chronic pain management involves the development and application of various interventions based on the complex neurobiological mechanisms of pain. These interventions target neuroplasticity and CNS changes, aiming for long-term pain control and functional recovery [27]. Central sensitization, commonly observed in chronic pain patients, encompasses neuroplastic changes in the spinal dorsal horn and higher CNS structures, leading to a lowered pain threshold, amplified pain signals, and expanded pain perception areas [7, 17].
PNE is an educational intervention designed to explain the biological and physiological processes of pain in an accessible manner for patients [9]. Its primary goal is to reduce misconceptions and fear associated with pain while enhancing patients’ self-efficacy in managing their condition. Neuroimaging studies indicate that PNE alters activation patterns in the prefrontal cortex and limbic system, leading to the reorganization of pain perception and processing pathways [8, 28].
Key educational topics in PNE include the biopsychosocial model of pain, the concept of central sensitization, the relationship between pain and tissue damage, and the neuroplasticity of the nervous system [29]. Recent studies have demonstrated PNE’s effectiveness across various chronic pain conditions, such as chronic low back pain, fibromyalgia, and chronic widespread pain [9–12, 30]. The educational process employs tools like visual metaphors, real-life examples, and interactive explanations to enhance patient comprehension and engagement [31].
Understanding the structural and functional brain changes in chronic pain patients forms the basis of therapeutic approaches. Changes in executive function within the prefrontal cortex influence decision-making and behavior regulation [32], while hyperactivation of the amygdala heightens anxiety and fear responses related to pain [33]. Alterations in self-referential processing in the posterior cingulate cortex affect the personal meaning and interpretation of pain, and changes in the insula modulate interoception and pain perception [34, 35].
These neurological changes are reversible, and appropriate interventions can reconfigure them positively [5]. Structural and functional connectivity changes in the brain are considered critical mechanisms in pain chronification, offering new therapeutic targets [18].
CFT is an integrated approach that addresses pain-related neurological changes through cognitive restructuring, behavior modification, and movement retraining [36]. CFT aims to identify and correct maladaptive beliefs, fear-avoidance behaviors, and dysfunctional movement patterns in patients [37].
The therapy comprises three main stages: first, understanding and evaluating individual factors related to the patient’s pain experience; second, modifying maladaptive behaviors and beliefs; and third, relearning functional activities and movements [38]. During the movement retraining phase, improvements in motor cortex reorganization and functional connectivity in sensory processing regions are observed [39, 40].
Mindfulness-based interventions emphasize nonjudgmental attention to present experiences, effectively modulating emotional and cognitive responses to pain [41]. fMRI studies show that mindfulness practice regulates activation in the anterior cingulate cortex and insula while enhancing top-down pain modulation networks [42].
Meditation and breathing techniques play a crucial role in balancing the autonomic nervous system and managing stress responses [43]. Practices such as slow breathing and mindfulness meditation regulate HPA axis activity, reducing pain sensitivity [44], leading to decreased cortisol levels and improved immune function [45]. These techniques are also effective in alleviating pain-related anxiety and depressive symptoms [46]. However, several limitations should be considered. Implementation challenges include variable patient engagement, resource constraints, and the need for specialized training. Additionally, the effectiveness of mindfulness interventions may vary significantly among different patient populations, and long-term adherence remains a concern.
Virtual reality and augmented reality technologies provide innovative approaches to pain management [47]. Beyond simple distraction, these technologies function as therapeutic tools by modifying somatosensory representations in the brain and facilitating motor relearning [48]. Neuroimaging studies reveal that VR interventions regulate activity in pain-related brain regions, particularly the anterior cingulate cortex, and insula while activating endogenous analgesic systems [49].
VR is especially effective in creating a safe environment that reduces fear of movement and encourages gradual engagement in physical activities for chronic pain patients [50]. AR, on the other hand, integrates therapeutic elements into real-world environments, enabling patients to adopt pain management strategies more effectively in daily life [51].
Motor imagery and graded motor imagery (GMI) are effective interventions that promote motor cortex reorganization without actual movement [52]. GMI consists of three progressive stages: laterality recognition, explicit motor imagery, and mirror therapy. Each stage incrementally activates neural networks involved in motor planning and execution [53]. These approaches have shown particular efficacy in managing chronic pain conditions such as complex regional pain syndrome [54].
Biofeedback and neurofeedback enable real-time monitoring and regulation of physiological states [55]. These techniques empower patients to self-regulate autonomic nervous system functions. For instance, electromyography biofeedback is effective in controlling muscle tension and reducing pain [56]. Neurofeedback directly targets pain processing networks by allowing patients to voluntarily modulate brainwave patterns, offering a novel avenue for intervention [57].
Body awareness techniques approach pain management by enhancing proprioception and interoception [58]. Methods such as the Alexander Technique and Feldenkrais Method emphasize strengthening the mind-body connection and correcting inefficient movement patterns [39]. These techniques have been shown to promote reorganization of the somatosensory cortex and normalization of body schema [8], improving body awareness and self-regulation in chronic pain patients [5].
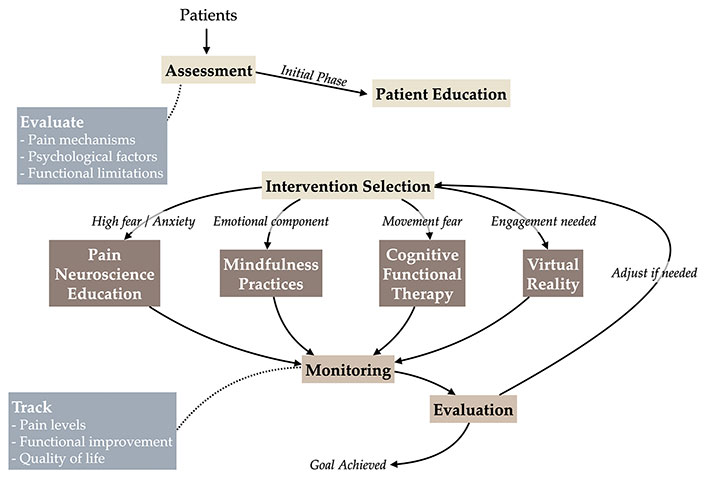
Effective chronic pain management necessitates the systematic clinical application of neuroscience-based interventions. Notably, the integration of multiple interventions has demonstrated superior therapeutic outcomes compared to single-modality approaches [59] (Figure 1).
Neuroscience-based interventions are more effective when combined with other therapeutic modalities. For instance, the combination of PNE with exercise therapy yields better results in pain reduction and functional improvement compared to each intervention alone [60]. Similarly, incorporating mindfulness or CFT into traditional physical therapy has been shown to enhance the reorganization of pain-related neural networks [61]. This multimodal approach addresses the multidimensional nature of chronic pain and promotes changes at various levels of the CNS [31]. Furthermore, recent studies suggest that integrating emerging technologies, such as virtual reality or biofeedback, with conventional treatments can enhance patient engagement and therapeutic outcomes [62].
To optimize the effectiveness of interventions, tailored approaches that consider individual patient characteristics and conditions are crucial. Assessing factors such as the degree of central sensitization, psychosocial influences, and cognitive receptiveness is essential in determining the appropriate combination of interventions [63]. Research shows that personalized approaches improve treatment efficacy and patient satisfaction [64]. Clinical decision-making should encompass not only the patient’s pain mechanisms but also functional demands in daily life, personal goals, and social support systems [4].
In clinical practice, systematic treatment algorithms are used to determine the sequence and intensity of interventions. Initial evaluations should comprehensively assess the neurobiological characteristics of pain, as well as the patient’s beliefs, expectations, and living environment [65]. Based on this, stepwise and progressive intervention plans are developed and continuously adjusted according to patient responses [66]. Regular re-evaluations and feedback during the treatment process are essential for monitoring intervention efficacy and refining therapeutic strategies as needed [67]. A clinical case study by Caneiro et al. [68] demonstrated the effectiveness of integrated neuroscience-based interventions in a 49-year-old patient with persistent low back pain. Similar to this case report, Fersum et al. [36] documented significant improvements in patients receiving CFT, with a mean pain reduction of 35–40%. The integration of PNE and mindfulness practices has also shown synergistic effects, as reported by Louw et al. [9] and Cherkin et al. [46].
Studies on the cost-effectiveness of neuroscience-based interventions are increasing. While these approaches may initially require more time and resources than traditional treatments, they contribute to long-term cost savings and improved quality of life [69]. Group-based programs and digital health technologies have gained attention as cost-effective delivery methods [70]. Additionally, integrating these interventions into primary care settings can enhance resource efficiency and accessibility, benefiting a broader range of patients [71].
Evaluating the effectiveness of interventions requires comprehensive outcome measures. Beyond traditional metrics such as pain intensity, assessments should include functional performance, quality of life, changes in pain perception, and neurophysiological markers [72]. Recently, the importance of patient-reported outcome measures has been emphasized, serving as valuable tools for assessing treatment efficacy and improving the quality of care [73].
The field of neuroscience-based interventions for chronic pain is rapidly evolving, offering both new opportunities and challenges for clinical practice and research [74]. Innovations in neuroimaging are enhancing the understanding of how these interventions work at the neurobiological level, paving the way for the development of more personalized and effective treatment strategies [75].
To improve the outcomes of chronic pain management, key research areas need further exploration. One priority is a detailed understanding of the mechanisms underlying individual interventions. For example, studies should investigate how educational approaches restructure pain-related neural networks and how these changes contribute to long-term pain relief [21]. Longitudinal studies using advanced neuroimaging techniques could offer valuable insights into the dynamic effects of these interventions over time [19].
Another crucial focus is identifying the best combinations and sequences of interventions. While current evidence supports the effectiveness of multimodal approaches, additional research is required to establish detailed protocols [76]. Furthermore, studies should examine how specific intervention combinations may work differently based on individual patient profiles, such as their clinical presentation and psychosocial characteristics [63].
The integration of neuroscience-based interventions into clinical practice requires updated guidelines that reflect recent evidence. Standardized protocols and assessment tools are essential to facilitate effective implementation [4]. Many healthcare providers also need additional training to bridge the gap between the theoretical foundations of these approaches and their practical application, highlighting the importance of comprehensive education programs [68].
However, structural challenges in healthcare systems, including limited insurance coverage, resource constraints, and time pressures, often hinder the widespread use of these interventions [77]. Moreover, transitioning from traditional biomechanical models to modern neuroscience-based approaches demands significant shifts in mindset for both clinicians and patients, requiring careful planning and support [78].
Emerging digital health technologies offer promising solutions to many challenges in chronic pain management. Virtual reality and augmented reality are proving to be valuable tools for enhancing pain management, particularly by supporting motor relearning and modulating pain perception [79]. Large language model-based chatbots are emerging as innovative tools for providing personalized support and guidance to patients, offering round-the-clock assistance and adaptive pain management strategies [80]. The integration of gamification elements into digital health interventions has shown the potential in improving patient engagement and treatment adherence by making therapeutic activities more engaging and rewarding [81]. Mobile health applications and wearable devices also provide opportunities for real-time monitoring, feedback, and improved patient engagement, thereby fostering better self-management and adherence to treatment [82].
Artificial intelligence and machine learning technologies are increasingly being explored for their potential to create individualized treatment plans and predict patient outcomes [83]. Advanced brain-computer interfaces offer promising opportunities for tailoring rehabilitation programs by directly measuring neural responses and adapting interventions in real time [84]. Insights gained from analyzing large datasets may help identify subgroups of patients and guide the development of more tailored intervention strategies [85]. Additionally, telehealth platforms are expected to play a key role in improving access to interventions, addressing geographical barriers, and reaching underserved populations [86].
Advancements in the neuroscientific understanding of chronic pain have introduced new paradigms in rehabilitation interventions. Neuroscience-based approaches such as PNE, mindfulness, and CFT directly target the neurobiological mechanisms of chronic pain, enabling more effective pain management. These interventions go beyond symptom relief, focusing on regulating central sensitization, promoting neuroplasticity, and reorganizing the pain neuromatrix to support long-term pain management and functional recovery.
A notable aspect of these approaches is their incorporation of educational components, which help reshape patients’ understanding and perception of pain, leading to sustained outcomes. This highlights the importance of active patient involvement and self-management in chronic pain care. Furthermore, the integration of multiple interventions has been shown to be more effective than standalone treatments, reflecting the complex nature of chronic pain and the necessity for multifaceted strategies.
To optimize the clinical application of these interventions, further research and the development of standardized protocols are essential. The evolution of digital technologies is expected to enhance the delivery and monitoring of these interventions, making them more accessible and efficient. In conclusion, neuroscience-based interventions represent a critical milestone in the future of chronic pain management, offering a patient-centered and integrative approach that redefines the direction of rehabilitation practices.
CFT: cognitive functional therapy
CNS: central nervous system
fMRI: functional magnetic resonance imaging
GMI: graded motor imagery
HPA: hypothalamic-pituitary-adrenal
PNE: Pain Neuroscience Education
HK: Conceptualization, Methodology, Investigation, Resources, Writing—original draft, Writing—review & editing, Supervision. The author has read and approved the submitted version of the manuscript.
The author declares that there are no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Edoardo Piacentino ... Jean-Pierre Van Buyten
Marco Cascella ... Valentina Cerrone