Original Article
Original Article

Affiliation:
1Department of Oral Medicine and Periodontology, Faculty of Dentistry, The British University in Egypt, El Sherouk City 11837, Egypt
Email: Dalia.Ghalwash@bue.edu.eg
ORCID: https://orcid.org/0000-0003-2541-7243
Affiliation:
1Department of Oral Medicine and Periodontology, Faculty of Dentistry, The British University in Egypt, El Sherouk City 11837, Egypt
ORCID: https://orcid.org/0000-0002-2087-4712
Affiliation:
2Department of Oral Medicine and Periodontology, Faculty of Dentistry, Galala University, Suez 15888, Egypt
ORCID: https://orcid.org/0000-0001-5069-8257
Explor Med. 2025;6:1001286 DOI: https://doi.org/10.37349/emed.2025.1001286
Received: December 12, 2024 Accepted: February 07, 2025 Published: February 19, 2025
Academic Editor: Gaetano Isola, University of Catania, Italy
Aim: Although xerostomia, smell, and taste dysfunctions are prominent signs of COVID-19 infection, long-term data regarding their prevalence and recovery rates is scarce. Accordingly, this study aimed to evaluate the frequency and persistence of xerostomia, taste, and smell disturbances in COVID-19 survivors over 3 years in an Egyptian sample.
Methods: This cross-sectional study used an online questionnaire to assess the oral symptoms of xerostomia, which include altered taste and smell. Data was collected from 826 patients recovered from COVID-19.
Results: Xerostomia was the most frequent finding affecting 73.6% of the studied sample, followed by smell disturbances affecting 67.8%, and altered taste reported by 54.6%. Xerostomia lasted less than 1 year in 48.3% of cases, up to 2 years in 10.4%, and up to 3 years in 7.2% of the study sample. Altered taste lasted less than 1 year in 77.8% of cases, up to 2 years in 2%, and up to 3 years in 0.4% of the study sample. Smell disturbances lasted around 1 month in 62.1% of cases, from 2–3 months in 36.1%, up to 1 year in 1.6%, and up to 2 years in 0.2% of the study sample. Xerostomia altered taste and smell, which impaired the quality of life and was more frequently observed in females than in males in the studied sample.
Conclusions: COVID-19 has a major and long-term impact on oral health, with frequent, intense, and longstanding oral symptoms that may impair a patient’s quality of life.
The global coronavirus pandemic of 2019 (COVID-19) has been associated with various clinical symptoms, including respiratory, cardiovascular, neurological, muscular, gastrointestinal, and chemosensory disorders [1, 2].
Additionally, oral manifestations are progressively evident in COVID-19-affected individuals [3]. Amongst clinical manifestations, are alterations in salivary secretion resulting in hyposalivation and xerostomia, taste, and smell dysfunction, about two-thirds of COVID-19 patients have at least one oral symptom [3, 4]. Reduced salivary flow negatively influences oral health conditions and quality of life and has also been proposed as a possible risk for COVID-19 illness [5, 6].
Various microbiota coexist in the human body and any dysbiosis of microbiota residing in the oral and nasal mucosal surfaces, causes immune modulation and several dysfunctions. The nasal microbiota modulates the physiology of the olfactory epithelium and causes inflammation, olfactory impairment, and even temporary or permanent olfactory dysfunction [7]. The composition of oral microbiota has been significantly associated with taste sensitivity, in addition to modulation of the host chemosensory functions by altering taste receptor density, promoting the secretion of inflammatory cytokines by host cells, and triggering inflammation [8].
COVID-19 virus attaches to angiotensin-converting enzyme 2 (ACE2) cell receptors to enter the targeted cells with subsequent priming of viral spike. ACE2 is expressed in epithelial cells of gingiva and taste cells in the dorsal surface of the tongue [9]. ACE2 is also expressed in parotid, submandibular, and minor salivary glands, indicating that they can act as reservoirs for viral particles that would be released through salivary ducts leading to high salivary viral loads in COVID-19 patients [9, 10]. Moreover, ACE2 is also highly expressed in the oral and olfactory epithelium targeted by SARS-CoV-2; thus COVID-19 is presumed to affect taste and smell functions and salivary secretion [9, 11].
Taste alterations were reported to be more frequent than smell dysfunction in several investigations [12, 13]. Nonetheless, most related studies have focused on olfactory dysfunction more than gustatory dysfunction [14]. Even though hyposalivation is not life-threatening it has negative effects on oral health and the quality of life in those patients as saliva is essential for proper taste function, swallowing, mastication, and speech [15, 16]. Thus, xerostomia leads to taste impairment, dysphagia, mastication problems, malnourishment, speech difficulty, increased dental caries, periodontitis, halitosis, oral candidiasis, and oral ulcers [17, 18].
Although most patients recover completely within a few weeks after COVID-19 infection, some people experience persistent symptoms after the acute stage of infection has passed, known as post-COVID-19 symptoms [19, 20].
Even though COVID-19-related clinical symptoms were recently reported in several studies, to the best of the author’s knowledge no studies have investigated the recovery rate of COVID-19-related clinical symptoms years after recovery especially in Egypt. Thus, the current study aimed to assess the frequency and persistence rate of self-reported COVID-19-associated xerostomia, taste, and smell disturbances in COVID-19 survivors up to 3 years of recovery in a sample of the Egyptian population.
This study evaluated the frequency and persistence of xerostomia, taste, and smell disturbances in COVID-19 survivors over 3 years in a sample of the Egyptian population.
Based on research published regarding the incidence of altered taste in the Egyptian population [21] by fixing alpha at 0.05 and beta at 0.2 the incidence of taste alteration associated with sex was 70% in females and 77% in males. The effective size g is 0.05 and the minimal sample size to be included is 826.
In a cross-sectional survey-based study, data was collected from 826 patients who suffered and/or recovered from COVID-19 who were recruited consecutively from the diagnostic center at The British University in Egypt from July 2023 till July 2024. Google Forms were used to develop an online questionnaire specifically designed for this study based on modified versions of the xerostomia questionnaire and the NHANES taste and smell questionnaire [22] (Supplementary material), it was circulated amongst those who were infected and/or recovered from coronavirus infection with different symptoms that, based on the evidence, could be linked to COVID-19. All patients were questioned about symptoms of xerostomia, taste, and smell disturbances. The online questionnaire was delivered in person during their visit to the diagnostic center, it included a total of 21 questions. Informed consent was obtained as the first question of the survey.
This cross-sectional survey-based study was approved by the Research Ethics Committee (REC 23-033), Faculty of Dentistry, The British University in Egypt, and all patients approved to participate.
Inclusion criteria:
Egyptian adults more than 21 years
Patients of both genders
Adults who had an active COVID-19 and those who recovered from it
Exclusion criteria:
Children and adolescents along with those who were not infected with coronavirus were excluded.
Patients who refuse to participate in the study
Vulnerable groups such as mentally and physically handicapped individuals
The first part assessed the patient’s demographic information (gender and age) and tobacco consumption, and then medical conditions and long-term medications were assessed. Evaluation of COVID-19 status, severity, and duration since recovery was then recorded. The following sections focused on reporting the patients’ symptoms of xerostomia, taste, and smell disturbances with information on their duration, intensity, and their effect on the quality of life for those patients. Patients rated their level of xerostomia, taste, and smell disturbances on a 10-point scale (from 1 = absent to 10 = severe). They rated the effect of xerostomia, taste, and smell disturbances on their quality of life on a 10-point scale (from 1 = no effect on quality of life to 10 = worst possible effect on quality of life). Responses to the survey were recorded on an electronic spreadsheet for statistical analysis.
Data were analyzed using IBM SPSS version 23 for Windows, Armonk, NY, USA. Quantitative data (age, intensity of symptoms, impact of quality of life) were checked for normality using the Kolmogorov-Smirnov test and Q-Q plots. Age was normally distributed; thus, it was presented using mean and standard deviation while the others were not normally distributed and presented using median, minimum, and maximum mainly. All qualitative data was summarized using frequency and percentage. Bivariate analysis was done using. The independent t-test and Pearson Chi-Square test were used to analyze the differences in independent variables according to the occurrence of disturbances in oral symptoms and smell. Multivariable binary logistic regression was employed to assess the effect of demographic variables, smoking status, and medical condition on the occurrence of xerostomia, taste disturbances, and smell disturbances. All tests were two-tailed, and the significance level was set at p-value.
The present cross-sectional study collected data from 826 patients who suffered and/or recovered from COVID-19. The mean age of the study sample was 37.19 ± 14.30. Females represented 57.5% of the total sample. Most of the sample were nonsmokers (84.6%). Among the smokers, 57.5% smoked 20 or fewer cigarettes per day. Most of the study samples were otherwise healthy (77.4%), and only 28.2% were on long-term medications. All demographic data are presented in Table 1.
Characteristics of the study sample
| Parameters | n = 826 patients | |
|---|---|---|
| Age: Mean ± SD | 37.19 ± 14.30 | |
| Gender: n (%) | Males | 351 (42.5%) |
| Females | 475 (57.5%) | |
| Smoking: n (%) | No | 699 (84.6%) |
| Yes | 127 (15.4%) | |
| Smoking frequency among smokers: n (%) | ≤ 20 cigarettes/day | 73 (57.5%) |
| > 20 cigarettes/day | 54 (42.5%) | |
| Medical condition: n (%) | No | 639 (77.4%) |
| Yes | 187 (22.6%) | |
| Long-term medications: n (%) | No | 593 (71.8%) |
| Yes | 233 (28.2%) | |
SD: standard deviation
The severity and duration of COVID-19 illness were described in Table 2 showing that 26.9% of cases had mild severity, more than half of the study sample suffered from moderate COVID-19 symptoms (51.8%), while in 14.6% of cases, symptoms were severe and 6.7% of cases were critical. Most cases recovered from COVID-19 symptoms in the last 6 months (28.9%) followed by 2 years (23.1%), 3 years (19%), 1 year then less than 6 months.
Description of COVID-19 illness severity and duration since recovery
| Parameters | n = 826 patients | |
|---|---|---|
| Severity of past/present confirmed COVID-19 illness: n (%) | Mild | 222 (26.9%) |
| Moderate | 428 (51.8%) | |
| Severe | 121 (14.6%) | |
| Critical | 55 (6.7%) | |
| Time passed since recovery: n (%) | < 6 months | 99 (12.0%) |
| 6 months | 239 (28.9%) | |
| 1 year | 140 (16.9%) | |
| 2 years | 191 (23.1%) | |
| 3 years | 157 (19.0%) | |
The most frequent finding in patients after COVID-19 was xerostomia, which was reported by 73.6% of the study sample, while smell disturbances were reported by 67.8% and altered taste was reported by 54.6% of the study sample. The mean symptom intensity of xerostomia was 6.54 ± 2.25, for altered taste it was 7.86 ± 2.15, and 6.10 ± 2.18 for altered smell. Xerostomia lasted less than 1 year in 48.3% of cases, around 1 year in 34.1%, up to 2 years in 10.4%, and up to 3 years in 7.2% of the study sample. While altered taste lasted less than 1 year in 77.8% of cases, around 1 year in 19.7%, up to 2 years in 2%, and up to 3 years in 0.4% of the study sample as shown in Table 3.
Patients reported COVID-19-related xerostomia and altered taste symptoms
| Parameters | Xerostomia | Taste | |
|---|---|---|---|
| Presence of symptoms during illness: n (%) | No | 218 (26.4%) | 375 (45.4%) |
| Yes | 608 (73.6%) | 451 (54.6%) | |
| Intensity of symptoms | Mean ± SD | 6.54 ± 2.25 | 7.86 ± 2.15 |
| Median (Min–Max) | 6.00 (2.00–10.00) | 8.00 (2.00–10.00) | |
| Duration of symptoms | Less than 1 year | 294 (48.3%) | 351 (77.8%) |
| 1 year | 207 (34.1%) | 89 (19.7%) | |
| 2 years | 63 (10.4%) | 9 (2.0%) | |
| 3 years | 44 (7.2%) | 2 (0.4%) | |
| Impact on quality of life | Mean ± SD | 6.40 ± 2.36 | 7.79 ± 2.27 |
| Median (Min–Max) | 6.00 (1.00–10.00) | 8.00 (2.00–10.00) | |
SD: standard deviation
Regarding symptoms of smell disturbances, they lasted less than 1 month in 62.1% of cases, from 2–3 months in 36.1%, up to 1 year in 1.6%, and up to 2 years in 0.2% of the study sample. Altered taste, xerostomia, and smell impaired the quality of life with mean scores of 7.79 ± 2.27, 6.40 ± 2.36, and 6.85 ± 2.25 respectively as shown in Tables 3 and 4.
Patient’s reported COVID-19-related smell symptoms
| Parameters | Smell | |
|---|---|---|
| Presence of symptoms during illness: n (%) | No | 266 (32.2%) |
| Yes | 560 (67.8%) | |
| Intensity of symptoms | Mean ± SD | 6.10 ± 2.18 |
| Median (Min–Max) | 6.00 (1.00–10.00) | |
| Duration of symptoms | Less than 1 month | 348 (62.1%) |
| 2–3 months | 202 (36.1%) | |
| 1 year | 9 (1.6%) | |
| 2 years | 1 (0.2%) | |
| Impact on quality of life | Mean ± SD | 6.85 ± 2.25 |
| Median (Min–Max) | 7.00 (2.00–10.00) | |
SD: standard deviation
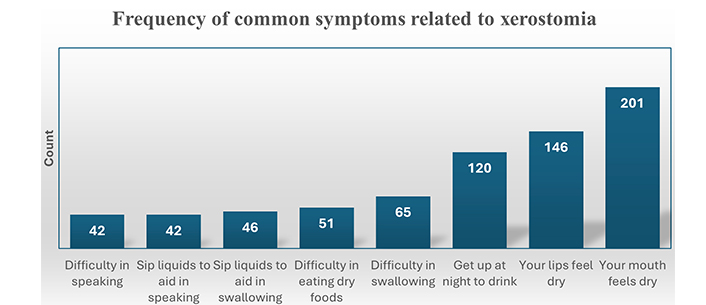
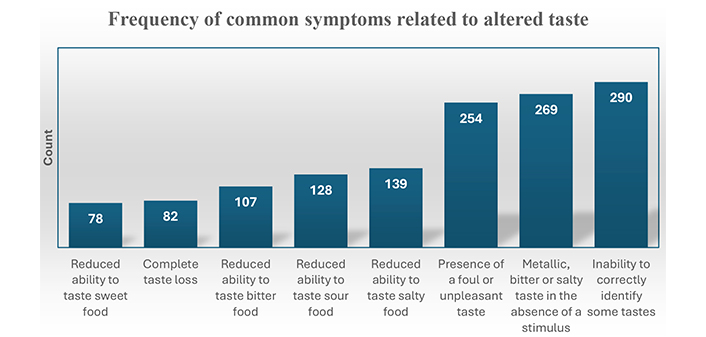
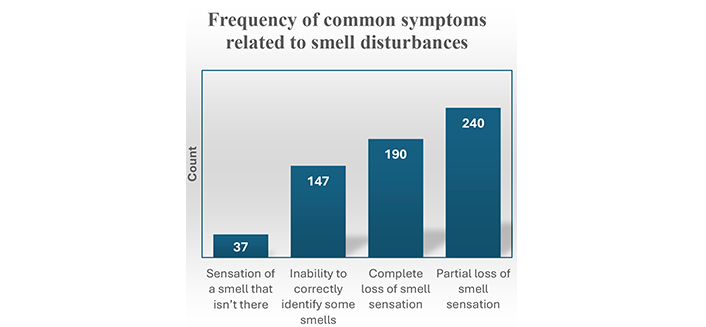
The most encountered xerostomia-related symptom was feeling the mouth dry followed by feeling the lips dry then getting up at night to drink. The frequency of common symptoms related to xerostomia is illustrated in Figure 1. The most encountered taste-related symptoms were the inability to correctly identify some tastes and metallic, bitter, or salty tastes in the absence of stimulus followed by the presence of foul or unpleasant tastes. The most common smell-related symptom was partial loss of smell followed by complete smell loss, then inability to correctly identify some smells. The frequency of common symptoms related to taste and smell disturbances are illustrated in Figures 2 and 3 respectively.
Taste, smell impairments, and xerostomia were more frequently observed in females than in males in the studied sample, and a significant difference was encountered in smell disturbance (p = 0.002*). There was also a significant association between altered taste, smell, and xerostomia with age, medical conditions, smoking, long-term medications, the severity of COVID-19 illness, and the time passed since recovery as presented in Table 5.
Association between COVID-19 illness severities with characteristics of the study sample
| Parameters | Xerostomia | Taste | Smell | ||||
|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | No | Yes | ||
| Age | Mean ± SD | 33.00 ± 12.46 | 38.70 ± 14.63 | 33.83 ± 12.69 | 39.99 ± 14.96 | 33.05 ± 12.43 | 39.16 ± 14.72 |
| p-value | < 0.0001* | < 0.0001* | < 0.0001* | ||||
| Gender: n (%) | Males | 101 (28.8%) | 250 (71.2%) | 169 (48.1%) | 182 (51.9%) | 134 (38.2%) | 217 (61.8%) |
| Females | 117 (24.6%) | 358 (75.4%) | 206 (43.4%) | 269 (56.6%) | 132 (27.8%) | 343 (72.2%) | |
| p-value | 0.182 | 0.173 | 0.002* | ||||
| Smoking: n (%) | No | 200 (28.6%) | 499 (71.4%) | 338 (48.4%) | 361 (51.6%) | 240 (34.3%) | 459 (65.7%) |
| Yes | 18 (14.2%) | 109 (85.8%) | 37 (29.1%) | 90 (70.9%) | 26 (20.5%) | 101 (79.5%) | |
| p-value | 0.001* | < 0.0001* | 0.002* | ||||
| Medical condition: n (%) | No | 185 (29.0%) | 454 (71.0%) | 314 (49.1%) | 325 (50.9%) | 229 (35.8%) | 410 (64.2%) |
| Yes | 33 (17.6%) | 154 (82.4%) | 61 (32.6%) | 126 (67.4%) | 37 (19.8%) | 150 (80.2%) | |
| p-value | 0.002* | < 0.0001* | < 0.0001* | ||||
| Long-term medication: n (%) | No | 172 (29.0%) | 421 (71.0%) | 295 (49.7%) | 298 (50.3%) | 216 (36.4%) | 377 (63.6%) |
| Yes | 46 (19.7%) | 187 (80.3%) | 80 (34.3%) | 153 (65.7%) | 50 (21.5%) | 183 (78.5%) | |
| p-value | 0.007* | < 0.0001* | < 0.0001* | ||||
| Severity of confirmed COVID-19 illness: n (%) | Mild | 120 (54.1%) | 102 (45.9%) | 162 (73.0%) | 60 (27.0%) | 124 (55.9%) | 98 (44.1%) |
| Moderate | 91 (21.3%) | 337 (78.7%) | 186 (43.5%) | 242 (56.5%) | 128 (29.9%) | 300 (70.1%) | |
| Severe | 7 (5.8%) | 114 (94.2%) | 25 (20.7%) | 96 (79.3%) | 14 (11.6%) | 107 (88.4%) | |
| Critical | 0 (0%) | 55 (100%) | 2 (3.6%) | 53 (96.4%) | 0 (0%) | 55 (100%) | |
| p-value | < 0.0001* | < 0.0001* | < 0.0001* | ||||
| Time passed since recovery: n (%) | < 6 months | 44 (44.4%) | 55 (55.6%) | 74 (74.7%) | 25 (25.3%) | 57 (57.6%) | 42 (42.4%) |
| 6 months | 91 (38.1%) | 148 (61.9%) | 137 (57.3%) | 102 (42.7%) | 93 (38.9%) | 146 (61.1%) | |
| 1 year | 27 (19.3%) | 113 (80.7%) | 58 (41.4%) | 82 (58.6%) | 41 (29.3%) | 99 (70.7%) | |
| 2 years | 40 (20.9%) | 151 (79.1%) | 74 (38.7%) | 117 (61.3%) | 46 (24.1%) | 145 (75.9%) | |
| 3 years | 16 (10.2%) | 141 (89.8%) | 32 (20.4%) | 125 (79.6%) | 29 (18.5%) | 128 (81.5%) | |
| p-value | < 0.0001* | < 0.0001* | < 0.0001* | ||||
* Statistically significant difference at p-value < 0.05
Most smokers reported xerostomia symptoms (p = 0.001*), most patients with long-term medication reported xerostomia (p = 0.007*), most cases were suffering from moderate severity of COVID-19 symptoms and all patients with critical symptoms suffered from xerostomia (p < 0.0001*). Also, time passed since recovery was significantly associated with xerostomia.
Taste disturbances were reported among older patients with a mean age of 39.99 ± 14.96 (p < 0.0001*). Most smokers and patients with medical conditions reported altered taste symptoms (p < 0.0001*), and most of the cases suffered from moderate severity of COVID-19 symptoms. Also, time passed since recovery was significantly associated with altered taste symptoms.
According to multivariable regression model, xerostomia was significantly associated with age with AOR = 1.03, p = 0.002*. Similarly, gender was significantly associated with xerostomia where females were more affected than males (AOR = 1.45, p = 0.038*). Also, being a smoker increased the risk of xerostomia occurrence by 2.47 times as compared to non-smokers. Similarly, taste and smell disturbances occurred more in older age, females, and smokers. On the other hand, medical conditions and medication were not significantly associated with either xerostomia, taste, or smell disturbances. Multivariable binary logistic regression assessing the effect of demographic variables, smoking status, and medical condition on the occurrence of xerostomia, taste disturbances, and smell disturbances are presented in Table 6.
Multivariable binary logistic regression assessing the effect of demographic variables, smoking status, and medical condition on the occurrence of xerostomia, taste disturbances, and smell disturbances
| Parameters | Age | Female vs. male | Smoking vs. no smoking | Medical condition vs. no medical condition | Long medication vs. no long medication | |
|---|---|---|---|---|---|---|
| Xerostomia | AOR | 1.03 | 1.45 | 2.47 | 1.07 | 0.96 |
| 95% CI | 1.01, 1.04 | 1.02, 2.05 | 1.39, 4.40 | 0.56, 2.03 | 0.55, 1.65 | |
| p-value | 0.002* | 0.038* | 0.002* | 0.838 | 0.871 | |
| Taste disturbances | AOR | 1.02 | 1.45 | 2.39 | 0.95 | 1.19 |
| 95% CI | 1.01, 1.04 | 1.05, 2.00 | 1.50, 3.82 | 0.54, 1.69 | 0.72, 1.95 | |
| p-value | < 0.0001* | 0.025* | < 0.0001* | 0.871 | 0.501 | |
| Smell disturbances | AOR | 1.02 | 1.90 | 2.45 | 1.13 | 1.19 |
| 95% CI | 1.01, 1.04 | 1.36, 2.65 | 1.46, 4.09 | 0.61, 2.11 | 0.69, 2.03 | |
| p-value | 0.005* | < 0.0001* | 0.001* | 0.691 | 0.533 | |
AOR: adjusted odds ratio; CI: confidence interval; * statistically significant difference at p-value < 0.05. Models’ summary: xerostomia (χ2 = 38.63, df = 5, p-value < 0.0001, –2 log likelihood = 914.78, Nagelkerke R Square = 0.067, percentage of correctly classified = 73.6%), taste disturbances (χ2 = 54.13, df = 5, p-value < 0.0001, –2 log likelihood = 1,083.94, Nagelkerke R Square = 0.085, percentage of correctly classified = 61.1%), smell disturbances (χ2 = 55.57, df = 5, p-value < 0.0001, –2 log likelihood = 982.533, Nagelkerke R Square = 0.091, percentage of correctly classified = 67.6%)
Since the emergence of the global COVID-19 pandemic, the focus has been directed to diagnosis, treatment, and preventive strategies for the disease. However, with the increase in the number the patients who survived COVID-19, various long-term effects of the disease became a highly imperative research area [23]. Bearing in mind the importance of xerostomia and chemosensory functions for safety and adequate quality of life [23], and the high global COVID-19 burden, it is imperative to pay more attention to the long-term frequency and persistence of such important COVID-19-associated oral complications, which are still not clear and under-investigated [24].
The current study aimed to estimate the frequency and persistence rate of self-reported COVID-19-associated xerostomia, smell, and taste disturbances in COVID-19 survivors up to 3 years of recovery in a sample of the Egyptian population. This investigation revealed that xerostomia was the most frequent finding affecting 73.6% of the studied sample, followed by smell disturbances reported by 67.8%. In comparison, altered taste was reported by 54.6%.
The prevalence of xerostomia is in the range or slightly higher than the rates stated by recent investigations reporting the occurrence of xerostomia in 47.6% of COVID-19 cases [25]. In another study, xerostomia was reported in 51.4% of patients [26]. Moreover, a recent meta-analysis reported a pooled xerostomia prevalence of 43% [27].
The prevalence of altered smell and taste found in the present study closely matches that reported by a large systematic review that assessed the prevalence of taste and smell disorders in 1,457 patients coming from different countries which reported a 60.7% prevalence rate of smell disfunction, and a 56.4% prevalence rate of disfunction [28].
Similarly, a different study conveyed that smell disturbance was the most common finding reported by 67% of patients followed by altered taste which was reported by 54.3% of patients, and xerostomia reported by 51.4% which corresponds to the present results [26]. Another study that assessed different symptoms in COVID-19 patients reported that smell disturbances affected 92%, taste disturbances were reported in 70% of patients which is higher than present data, while xerostomia was reported in only 32% of patients at a much lower rate than the present results [29]. Additionally, earlier research stated that altered taste was the most frequently recorded manifestation (59.5%), followed by xerostomia (45.9%) and altered smell (41.4%) [30], showing similar results of altered taste with a lower rate of xerostomia and altered smell compared to our results.
The variability in the prevalence rates of oral manifestations of COVID-19 may result from geographic location and ethnic differences. For instance, Asians and Africans were reported to be less prone to develop smell disturbances than Western populations following COVID-19 infection [31].
The co-occurrence of xerostomia altered taste and smell functions among COVID-19 cases encountered in the present study was also noticed in earlier research which reported the concurrence of xerostomia and altered taste function in many COVID-19 patients and suggested that altered taste function might be secondary to xerostomia or the other way around [32]. As taste substances first dissolve in saliva to interact with taste receptors to initiate the taste perception pathway and this would also stimulate salivary secretion by main salivary glands via the gustatory-salivary reflex which could be negatively affected by neuropathy of cranial nerves resulting from neuro-invasive COVID-19, inducing xerostomia, and altered taste function [33].
Additionally, alterations of salivary flow and salivary composition are known complications of COVID-19 infection which would eventually result in xerostomia and disturbance of taste function [34]. Olfactory disturbance frequently occurring because of COVID-19 infection may additionally contribute to xerostomia since the smell of food stimulates salivary secretion, with subsequent taste dysfunction. Moreover, xerostomia usually appears as a side effect of drugs used for various diseases including drugs used for treating COVID-19 itself [12].
In the presently studied sample xerostomia, smell, and taste disturbances were more often perceived by females, which is in accordance with prior research [4, 35, 36]. Additionally, in the present results, a significant association of smell disturbance with the female gender was encountered. This agrees with some studies declaring a higher prevalence of altered taste and smell in females compared to males in both Asian and European countries [35, 37–39]. Moreover, the prevalence of altered taste in COVID-19 cases was reported to be higher in females compared to males [1, 40]. Furthermore, an earlier study reported that xerostomia was noted in females (83.3%) more than males (16.7%) [41].
These gender-related variances could be attributed to the higher ACE2 levels and lesser pro-inflammatory cytokines as IL-6 levels in females following viral infections rendering them more susceptible to developing post-COVID taste and smell disturbances [42, 43]. Furthermore, stress, sleep, anxiety, and depressive disorders, are more frequent in females and might affect the perception of taste and smell [44]. This would explain the more prevalent post-COVID symptoms found in females observed in various studies [43, 45, 46]. Conversely, other studies did not report any association between altered taste function and gender [47].
In the present study xerostomia, altered taste, and smell were found to significantly impair the quality of life of COVID-19 patients with mean scores of 7.79 ± 2.27, 6.40 ± 2.36, and 6.85 ± 2.25 respectively which agrees with previous studies reporting the undesirable effect of loss of these important senses affecting the ability to detect gas leaks, recognize spoiled foods resulting in a higher risk of food poisoning and intoxication, which is frequently associated with depression and apprehension, compromising the quality of life [7, 48].
Although most COVID-19-related symptoms including xerostomia and altered taste and smell are usually transient in most patients, a proportion of them continue to report symptoms for a variable time after COVID-19 illness [24]. Altered taste is a highly frequent symptom that has been reported to persist long after recovery. And according to recent research loss of taste or smell was reported as the second most common persistent symptom after fatigue [19]. Other studies reported that some individuals also complain of persistent xerostomia [49, 50]. A recent meta-analysis reported a long-term prevalence of altered taste and smell of 14% and 15%, respectively, following COVID-19 [51].
The present study investigated the occurrence of clinical symptoms in COVID-19 survivors up to 3 years of recovery and revealed that xerostomia lasted less than 1 year in 48.3% of cases, around 1 year in 34.1%, up to 2 years in 10.4%, and up to 3 years in 7.2% of the study sample. There are very limited studies to compare our results with, however, in an earlier shorter-term research xerostomia was reported to last for more than 8 months following COVID-19 recovery [27].
In the current study altered taste lasted less than 1 year in 77.8% of cases, around 1 year in 19.7%, up to 2 years in 2%, and up to 3 years in 0.4% of the study sample, which shows longer lasting taste disturbance than that reported in a recent systematic review concluding that taste alteration lasted for one month in 78.8% of patients, two months in 87.7%, three months in 90.3% and for six months in 98.0%, with median recovery time of 12.4 days [52]. Another study showed that 7.0–8.6% of altered taste cases persisted or even worsened in one year [24].
Regarding smell disturbances, they lasted less than 1 month in 62.1% of cases, from 2–3 months in 36.1%, up to 1 year in 1.6%, and up to 2 years in only 0.2% of the study sample. This agrees with a recent systematic review which reported that smell disturbances lasted for one month in 74.1% of participants, for two months in 85.8%, for three months in 90.0%, and for six months in 95.7% of patients with a median recovery time of 14.9 days [52].
Our results are also comparable to previous research reporting the persistence of smell disturbances for about 4 to 6 months of hyposmia (53%), and anosmia (12%) [53, 54]. Besides, in other investigations, 70 to 80% of patients reported complete recovery from smell and taste disturbances within 1 to 2 months [55, 56]. On the other hand, a recent long-term study reported that up to 28% of post-COVID-19 patients displayed smell dysfunction for up to 2 years [24], contrary to the persistence of smell impairment for 2 years in only 0.2% of the present study sample.
Additionally, partial loss of smell sensation or hyposmia was reported in 39% of cases in the current investigation, while 31% suffered from complete loss of smell sensation or anosmia and 24% complained of inability to correctly identify some smells, whereas only 6% of cases reported phantosmia. These results are more or less in accordance with previous research where 34% of patients reported anosmia in a self-reported cross-sectional study in Italy [40], while a higher percentage was reported in another online survey [36].
Another survey registered that 68% of COVID-19 patients complained of different olfactory symptoms and that 71% suffered from taste dysfunctions [57]. Moreover, 35% of the patients reported anosmia before testing, though this percentage rose to 58% after performing validated smell tests demonstrating a difference between self-report rate and measured smell assessment which reflects that self-reported based studies could lead to underestimation of actual rates of taste and smell disturbances [14]. On the other hand, lower numbers were declared by another study reporting anosmia in only 19.5% of COVID-19 patients [26].
In the current investigation, there was a significant association between xerostomia, altered taste, and smell and age, medical conditions, and smoking. These findings follow a previous meta-analysis [31]; however, another systematic review did not find a relation between altered taste and smell and race, sex, medical conditions, or smoking [58].
A significant association was also found between the three conditions and the severity of COVID-19 illness where the most affected category was moderate followed by severe and mild illness and the least affected category was that of critical patients. This was in line with earlier research reporting that taste dysfunction was encountered less in critical and severe cases than in asymptomatic, mild, and moderate COVID-19 cases, however, they reported the highest association with relatively mild severity of COVID-19 not moderate [59].
Moreover, the persistence of altered taste and smell sensation for 6 months after COVID-19 was reported in 13.9% of patients with mild severity, 4.3% with moderate, 4.2% with severe, and 0% in critical cases showing that the severity of COVID-19 illness might govern the frequency and persistence of taste impairment [3]. These findings also suggest that critically and severely affected patients who exhibit less frequency of the studied symptoms and those with mild or moderate disease exhibiting higher symptom frequency might have different clinical courses or pathways of viral spread. Thus, altered taste and smell sensations might reveal prognostic indications of the disease severity besides being potential screening symptoms for COVID-19 infection [57].
The longer-lasting xerostomia, taste, and smell disturbances revealed in this study are most probably attributed to the longer period covered by this investigation since COVID-19 recovery. Addressing these long-term issues is essential to help COVID-19 survivors and improve their quality of life. An improvement in some cases even after long-term persistence of oral symptoms was noticed in the current study, following data analysis of recent studies that reported complete recovery after 3 years in one-third of the subjects who reported persistent symptoms. These findings confirm that the recovery of xerostomia taste and smell functions even after many years remains possible [24, 35]. Therefore, COVID-19 patients require timely identification, and close monitoring and should be followed up over the long term.
In the current study oral symptoms were self-reported via cross-sectional surveys, which may be considered a limiting factor in terms of sensitivity. Thus, oral symptom frequency could be underrated compared to studies depending on physical examination and accurate assessment methods. However, self-reported outcomes are best reflective of the patient’s perception. Another limitation is this study’s retrospective nature, which could be subjected to recall bias. Thus, additional long-term prospective studies are encouraged. Additionally, the possible effect of vaccinations and therapies administered to patients for COVID-19 treatment on the rate, severity, and persistence of oral and clinical symptoms needs to be investigated in future research.
COVID-19 has a major and long-term impact on oral health, with frequent, intense, and longstanding oral symptoms that may impair the quality of life. Xerostomia was the most frequent finding, affecting 73.6% of post-COVID-19 patients, followed by smell disturbances, affecting 67.8%, and then altered taste, which was reported by 54.6% of the studied sample. Xerostomia, altered taste, and smell were more significantly associated with age, female gender, and smoking.
ACE2: angiotensin-converting enzyme 2
COVID-19: global coronavirus pandemic of 2019
The supplementary material for this article is available at: https://www.explorationpub.com/uploads/Article/file/1001286_sup_1.pdf.
We would like to acknowledge the contributions of the oral diagnosis specialists for helping us with data collection throughout the study.
DG: Conceptualization, Investigation, Writing—review & editing. AAB: Investigation, Visualization. AH: Investigation, Writing—original draft. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
Approval was obtained from the Research Ethics Committee, Faculty of Dentistry, The British University in Egypt with approval No. (REC 23-033).
The procedures were fully explained to the patients, and they signed an informed consent to share their clinical data for scientific purposes.
Not applicable.
The data that support the findings of this study are available from the oral diagnosis center at The British University in Egypt and restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data, however, is available from the corresponding author upon reasonable request.
Not applicable.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.