Case Report
Case Report

Affiliation:
1Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
2Center for Basic and Clinical Immunology Research (CISI), University of Naples Federico II, 80131 Naples, Italy
3World Allergy Organization (WAO) Center of Excellence, 80131 Naples, Italy
ORCID: https://orcid.org/0000-0002-4723-0167
Affiliation:
1Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
ORCID: https://orcid.org/0000-0002-6434-3112
Affiliation:
1Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
ORCID: https://orcid.org/0009-0004-4664-2348
Affiliation:
1Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
ORCID: https://orcid.org/0009-0000-6163-3213
Affiliation:
1Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
ORCID: https://orcid.org/0009-0002-3782-6036
Affiliation:
1Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
ORCID: https://orcid.org/0009-0001-3053-464X
Affiliation:
1Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
ORCID: https://orcid.org/0000-0002-5781-2865
Affiliation:
1Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
2Center for Basic and Clinical Immunology Research (CISI), University of Naples Federico II, 80131 Naples, Italy
4Interdepartmental Center of Clinical and Translational Sciences (CIRCET), University of Naples Federico II, 80131 Naples, Italy
5Interdepartmental Hypertension Research Center (CIRIAPA), University of Naples Federico II, 80131 Naples, Italy
ORCID: https://orcid.org/0000-0001-5983-688X
Affiliation:
1Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
2Center for Basic and Clinical Immunology Research (CISI), University of Naples Federico II, 80131 Naples, Italy
3World Allergy Organization (WAO) Center of Excellence, 80131 Naples, Italy
ORCID: https://orcid.org/0000-0003-0347-2540
Affiliation:
1Department of Translational Medical Sciences, University of Naples Federico II, 80131 Naples, Italy
2Center for Basic and Clinical Immunology Research (CISI), University of Naples Federico II, 80131 Naples, Italy
3World Allergy Organization (WAO) Center of Excellence, 80131 Naples, Italy
6Institute of Experimental Endocrinology and Oncology (IEOS), National Research Council, 80131 Naples, Italy
Email: gildanet@gmail.com
ORCID: https://orcid.org/0000-0002-9285-4657
Explor Med. 2025;6:1001294 DOI: https://doi.org/10.37349/emed.2025.1001294
Received: November 12, 2024 Accepted: February 26, 2025 Published: March 13, 2025
Academic Editor: Andrea Nicolini, University of Pisa, Italy
The article belongs to the special issue Breast Cancer: Basic and Clinical Advances
The advent of immunotherapy has revolutionized the therapeutic landscape of breast cancer. The immune checkpoint inhibitor drug, pembrolizumab, a monoclonal antibody targeting programmed cell death protein 1 (PD-1), was recently approved by the Food and Drug Administration (FDA) as a neoadjuvant treatment in combination with traditional chemotherapy in locally advanced triple-negative breast cancer (LA-TNBC). This manuscript aims to highlight an uncommon adverse event of immune checkpoint inhibitors (ICIs): hypereosinophilia (HE). Herein, we report the case of AW, a 49-year-old female patient, who was treated for triple-negative breast cancer (TNBC) with pembrolizumab, achieving a complete response. After undergoing surgery, pembrolizumab was reintroduced as adjuvant therapy, at which point an abnormal increase in eosinophil count was observed. Hence, treatment was interrupted, and after glucocorticoid administration, the eosinophil count reverted to normality. Our findings underscore the necessity for vigilant monitoring of blood eosinophil levels during pembrolizumab therapy and provide insights into the management of such immunotherapy-related adverse events.
Immune checkpoint inhibitors (ICIs) are monoclonal antibodies (mAbs) that block inhibitory molecules involved in the regulation of immune pathways, such as cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), programmed cell death protein 1 (PD-1), or its ligand programmed cell death protein ligand 1 (PD-L1) in the tumor microenvironment, which leads to systemic immune cell activation [1]. Pembrolizumab, a humanized IgG4 kappa anti-PD-1 mAb, has been extensively investigated in several malignancies, including melanoma, non-small cell lung cancer (NSCLC), and lymphomas [2]. PD-1 is a cell surface receptor expressed on T cells, B cells, and macrophages after they have been activated [3]. The primary ligands for PD-1 are PD-L1 and PD-L2, which both belong to the B7 family. When PD-1 binds to its ligands, it inhibits the proliferation of T cells, reduces cytokine production, and can lead to the apoptosis of antigen-specific T cells while promoting the survival of regulatory T (Treg) cells [4]. This interaction is an essential component of the immune response that helps prevent tissue damage during inflammation and maintain tolerance to self-antigens. However, many cancer cells exploit this regulatory pathway to evade immune detection and consequent destruction [5].
Immunotherapy strategies targeting the PD-1/PD-L1 axis have been developed to block this interaction, thereby enhancing the immune system’s ability to fight cancer [6]. Pembrolizumab has shown promising results in locally advanced triple-negative breast cancer (LA-TNBC). Recently, the Food and Drug Administration (FDA) approved its use in combination with chemotherapy as a neoadjuvant treatment, followed by adjuvant monotherapy post-radical surgery in patients with high-risk LA-TNBC [7, 8]. Despite its efficacy, pembrolizumab is associated with a spectrum of immune-related adverse events (irAEs) [9, 10] among which hypereosinophilia (HE) remains rare but significant [11, 12]. This case report highlights the critical need for awareness and understanding of such irAEs to optimize patient care.
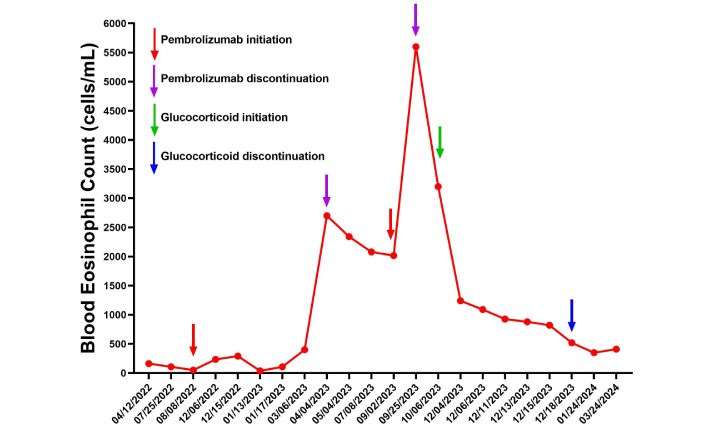
AW, a 49-year-old woman with a history of hypothyroidism, bronchial asthma, and allergic rhinitis, was diagnosed with LA-TNBC in March 2022. From 17 August 2022 to 6 March 2023, she underwent neoadjuvant chemotherapy with carboplatin and paclitaxel on weekly administrations for 12 cycles, supplemented by pembrolizumab (200 mg e.v. every 3 weeks), followed by 4 cycles of epirubicin and cyclophosphamide in addition to pembrolizumab. In April 2023 she underwent a left total mastectomy with left axillary lymph node dissection, achieving pathological complete response (ypT0N0). From 29 June 2023 to 18 July 2023, the patient underwent adjuvant radiotherapy. Concurrently, the medical treatment plan incorporated the prosecution of nine cycles of immunotherapy with pembrolizumab. Table 1 represents a timetable in which are displayed radiological findings and biopsy reports from the time of disease detection through neoadjuvant medical treatment, surgery, and adjuvant radiotherapy. Pembrolizumab administration was halted on August 14th, 2023, following the identification of persistent and progressive eosinophilia (initial eosinophil count: 0.4 × 103 cell/µL; peak value 5.6 × 103 cell/µL), as illustrated in Figure 1. Therefore, she was admitted to the Clinical Immunology Division of the University of Naples Federico II on December 4th, 2023, where further diagnostic tests were performed to rule out primary and secondary causes of HE. The patient was apparently asymptomatic except for worsening of her diagnosed bronchial asthma. Furthermore, there was no evidence of systemic involvement on physical examination.
Timetable of radiological imaging and biopsy reports over the time from disease detection
| Date | Imaging/Procedure | Summary |
|---|---|---|
| 17/03/2022 | Breast US | Dense glandular tissue, fibrocystic mastopathy. Suspicious left axillary lymph node (22 × 20 mm). |
| 18/03/2022 | Mammography | Dense parenchyma with nodular aspects, no pathological calcifications. Axillary lymph nodes present. |
| 07/04/2022 | Axillary core biopsy | Poorly differentiated carcinoma with squamous features. |
| 19/04/2022 | Breast MRI | Large heterogeneous lesion in left breast (> 42 mm), enlarged left axillary lymph node (> 45 mm), BIRADS 5. |
| 19/04/2022 | Full-body CT scan | Enlarged left axillary lymph nodes, small liver and ovarian cysts, mild left pleural effusion. |
| 18/05/2022 | PET scan | Pathological hyperaccumulation in left breast (SUVmax 6.3), bilateral lymph node involvement. Indeterminate pelvic lesion. |
| 20/05/2022 | Abdomen US | Hepatomegaly with small angioma (5 mm), distended gallbladder, no peritoneal fluid. |
| 01/06/2022 | Mammary and axillary biopsy | High-grade invasive carcinoma (ER–/PR–/HER2–, Ki-67 40%). Lymph node involvement confirmed. |
| 14/08/2022–06/03/2023 | Neoadjuvant chemotherapy | Carboplatin/paclitaxel + pembrolizumab (12 cycles), followed by epirubicin/cyclophosphamide + pembrolizumab (4 cycles). |
| 12/12/2022 | Mammography | Reduction in left breast mass (19 mm vs 33 mm), persistent axillary lymphadenopathy. |
| 09/12/2022 | Full-body CT scan | Stable mammary and lymph node lesions. Ascending aortic aneurysm (42 mm). |
| 13/03/2023 | Abdomen US | Small gallbladder adenomyoma (5 mm). |
| 14/03/2023 | Breast US | Left fibroadenoma (15 mm), reactive axillary lymphadenopathy bilaterally. |
| 27/03/2023 | PET scan | Stable left breast lesion improved axillary lymph nodes. |
| 29/03/2023 | Breast MRI | Persistent left breast nodules (12 mm vs 15 mm), BIRADS 6. |
| 14/04/2023 | Left total mastectomy and axillary dissection | Fibrocystic changes. Negative margins. 10 lymph nodes disease-free. Pathological stage: ypT0N0. |
| 29/06/2023–18/07/2023 | Radiotherapy | 42.56 Gy to left breast, supraclavicular/subclavian nodes, and internal mammary chain. Mild skin toxicity (G1). |
| 29/06/2023–04/08/2023 | Immunotherapy | Pembrolizumab. |
| 14/10/2023 | Breast US | Post-mastectomy changes. Right breast with cystic and dysplastic nodules. Normal lymph nodes. |
| 24/10/2023 | Full-body CT scan | Mild pulmonary changes, left mastectomy without recurrence, hepatomegaly. |
US: ultrasound; BIRADS: breast imaging reporting and data system
Immunophenotype and genetics for FIP1L1-PDGFRA were performed, both resulting in negative; stool test and parasitological fecal examination on three specimens for eggs and parasites were also negative. Serum IgG for Strongyloides stercoralis, serum antigen of Cryptococcus neoformans, Aspergillus galactomannan antigen, and serum Quantiferon test ruled out infectious causes of HE. Liver function tests, cortisol levels, and vitamin B12 levels were also normal. A cardiac ultrasound, cardiac enzymes, and electrocardiogram revealed no abnormalities. The patient also underwent bone marrow aspiration and biopsy, which showed trilinear, normo-cellular marrow with a prominent proportion of eosinophilic granulocytes. During hospitalization, the eosinophil blood count value was consistently elevated despite discontinuation of pembrolizumab. Given the negativity of all the diagnostic and instrumental tests performed, she was discharged with a diagnosis of pembrolizumab-related HE and an indication to start therapy with prednisone 25 mg per day with progressive tapering into 2 weeks. Monthly peripheral blood eosinophil counts were performed after the discontinuation of the glucocorticoid therapy and showed a normalization of blood eosinophil levels from one month after hospital discharge, with collateral improvement in the symptoms of bronchial asthma.
ICIs provide clinical benefit in a percentage of patients with advanced cancer, but they are usually associated with a remarkable spectrum of irAEs [9, 10, 13]. Although any organ system can be involved, hematological irAEs such as anemia, thrombocytopenia, and neutropenia are less frequently observed [14]. Nevertheless, some cases of ICI-induced HE have been documented across different malignancies, underlining the need for vigilance [15]. Most irAEs resolve either pharmacologically or after discontinuation of ICIs, but some appear to be persistent. Glucocorticoids are the mainstay of irAEs management [16]. However, other immunosuppressive drugs can be used to treat refractory irAEs [17].
Eosinophilia is defined as a peripheral blood eosinophil count above the upper limit of normal, which typically represents 3–5% of peripheral leukocytes, translating to an absolute eosinophil count (AEC) of 0.35–0.5 × 109/L [18]. The severity of eosinophilia is stratified into mild (AEC up to 1.5 × 109/L), moderate (AEC 1.5–5 × 109/L), and severe (AEC > 5 × 109/L). HE is, therefore, clinically established upon detection of an AEC exceeding 1.5 × 109/L on two distinct occasions, separated by a minimum time frame of one month [18]. HE includes a broad range of non-hematologic (secondary or reactive) and hematologic (primary or clonal) disorders with the potential for end-organ damage. Essentially, all organ systems can be susceptible to prolonged eosinophilia [19]. Dermatological involvement is the most common clinical manifestation reported in 69% of patients, followed by pulmonary (44%) and gastrointestinal (38%) manifestations. Cardiac disease unrelated to hypertension, atherosclerosis, or rheumatic disease has been identified in 20% of patients [20]. In a study involving 146 patients receiving various ICIs, including pembrolizumab, eosinophilia developed in 22% of patients during treatment [21]. Few cases of eosinophilia associated with pembrolizumab administration have been described in the literature. Baroz et al. [22] highlighted that pembrolizumab, used as a first-line systemic therapy in patients with NSCLC, can lead to high blood eosinophil counts. Furthermore, Soto and collaborators [23] described a case of eosinophilia associated with severe asthma and sarcoidosis one month after starting pembrolizumab for metastatic nasopharyngeal carcinoma, successfully treated with interleukin-5 (IL-5) inhibition. Harada et al. [24] have recently reported a case of asthma exacerbation with HE and elevated serum IL-5 in a patient undergoing pembrolizumab therapy for endometrial cancer. Khoja et al. [25] also observed eosinophilia in association with eosinophilic fasciitis and acute encephalopathy toxicity due to pembrolizumab used for the treatment of metastatic melanoma. HE can occur even months after the start of pembrolizumab treatment, as reported in this case.
To our knowledge, this report is the first documentation of pembrolizumab-induced HE in the context of LA-TNBC. This case underlines the imperative for clinicians to maintain a high index of suspicion for this rare but significant adverse effect.
The pathophysiological mechanisms underlying pembrolizumab-associated HE remain largely unknown, but several hypotheses have been proposed. One potential explanation involves the disruption of immune homeostasis due to PD-1 blockade, leading to an unregulated activation of eosinophils. PD-1 plays a critical role in maintaining immune tolerance, and its inhibition may result in excessive T-cell activation, particularly Th2-mediated immune responses, which promote eosinophil recruitment and activation. Additionally, pembrolizumab-induced HE may be linked to increased levels of IL-5, a key cytokine in eosinophil proliferation and survival, as observed in prior reports of pembrolizumab-related eosinophilic complications. The tumor microenvironment, particularly in highly immunogenic cancers such as TNBC, may also contribute to this phenomenon by altering the immune landscape following neoadjuvant chemotherapy and immunotherapy. Changes in cytokine profiles and immune cell infiltration, including shifts in tumor-infiltrating lymphocytes (TILs), may play a role in the development of HE as an irAE. Future studies investigating cytokine signatures and immune cell dynamics in patients receiving ICIs could provide further insight into the mechanisms responsible for pembrolizumab-induced HE.
The management of pembrolizumab-induced HE requires its discontinuation as the first intervention. If eosinophilia persists despite discontinuation of the drug, treatment with glucorticoids is necessary. As shown in our case, glucorticoid therapy caused a rapid reduction of peripheral blood eosinophils. Published guidelines from the National Comprehensive Cancer Network (NCCN) [26], European Society for Medical Oncology (ESMO) [27], and American Society of Medical Oncology (ASCO) [28] outline recommendations for the management of immunotherapy-induced HE. These guidelines emphasize the importance of regular monitoring of eosinophil counts, early recognition of eosinophilia, and comprehensive evaluation to rule out secondary causes such as infections, hematologic malignancies, or autoimmune conditions. In cases of mild or asymptomatic HE, close observation is suggested, whereas moderate to severe eosinophilia, particularly if accompanied by organ involvement, necessitates immediate intervention with high-dose corticosteroids. In refractory cases, additional immunosuppressive therapies such as IL-5/IL-5Rα inhibitors, including mepolizumab or benralizumab, may be considered. Reintroduction of pembrolizumab may be cautiously attempted following resolution of HE, but recurrence mandates permanent discontinuation. These recommendations align with our management approach, reinforcing the need for vigilance in monitoring immune-related hematological toxicities and the role of immunosuppressive therapies in mitigating these adverse effects.
TNBC is known for its high immunogenicity, which contributes to its responsiveness to immunotherapy and neoadjuvant chemotherapy. This is partly due to the presence of elevated TILs, which have been associated with improved clinical outcomes and a higher likelihood of achieving pathological complete response [29]. Neoadjuvant chemotherapy can induce modifications in the tumor immune microenvironment, potentially influencing both treatment efficacy and the development of irAEs. Although in our case TIL density and PD-1/PD-L1 expression were not assessed before or after treatment, future studies incorporating these biomarkers could provide valuable insights into the mechanisms underlying both treatment response and immunotherapy-related toxicities.
In conclusion, our case report illustrates a rare late onset of HE associated with pembrolizumab in the treatment of early LA-TNBC. This case highlights the need for awareness among clinicians regarding potential hematological side effects of ICIs. The lack of resolution of HE following discontinuation of pembrolizumab and the need of glucocorticoid therapy suggests a manageable approach to this adverse event. HE requires specific treatment, as it can be associated with cardiovascular, neurologic, and thrombotic events [30, 31]. Therefore, clinicians should consider HE as a possible side effect associated with pembrolizumab therapy. This report adds to the growing evidence on ICI safety profiles and calls for further research to elucidate the mechanisms underlying such immune-mediated adverse events.
AEC: absolute eosinophil count
HE: hypereosinophilia
ICIs: immune checkpoint inhibitors
IL-5: interleukin-5
irAEs: immune-related adverse events
LA-TNBC: locally advanced triple-negative breast cancer
mAbs: monoclonal antibodies
NSCLC: non-small cell lung cancer
PD-1: programmed cell death protein 1
PD-L1: programmed cell death protein ligand 1
TILs: tumor-infiltrating lymphocytes
The authors thank Dr. Gjada Criscuolo for her excellent managerial assistance in preparing this manuscript and the administrative staff (Dr. Roberto Bifulco, Dr. Anna Ferraro, and Dr. Maria Cristina Fucci), without whom it would not be possible to work as a team.
RP, AC, CGT, AdP, and GV: Conceptualization, Investigation, Writing—original draft, Writing—review & editing, Validation, Supervision. AdS, LS, ES, MTN, and MW: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
The research complies with the Declaration of Helsinki. This case report does not require ethical approval according to the requirements of the author’s country or institution.
Informed consent to participate in the study was obtained from the participant.
Informed consent to publication was obtained from the participant.
Datasets generated by this study are available upon request from the author (gildanet@gmail.com).
This work was supported in part by grants from the CISI-Lab Project (University of Naples Federico II), TIMING Project and Campania Bioscience (Regione Campania), and MIUR-PRIN 2017M8YMR8_005. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
© The Author(s) 2025.
Open Exploration maintains a neutral stance on jurisdictional claims in published institutional affiliations and maps. All opinions expressed in this article are the personal views of the author(s) and do not represent the stance of the editorial team or the publisher.
Copyright: © The Author(s) 2025. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
View: 4119
Download: 31
Times Cited: 0
Ali Abdul Hussein S. AL-Janabi ... Abdul Razzak Kalaf Hassan
Danila Coradini, Federico Ambrogi
Banashree Bondhopadhyay ... Vishakha Kasherwal
Nadia Islam, Suneela Vegunta
Spoorthi Marada ... Yi Lu
Danila Coradini
Kaoutar Anouar Tadlaoui ... Moulay Mustapha Ennaji