Original Article
Original Article

Affiliation:
1Department of Rheumatology, VieCuri Medical Centre, 5912BL Venlo, The Netherlands
2Departament of Rheumatology, University of Medicine and Pharmacy “luliu Hatieganu”, 400012 Cluj-Napoca, Romania
Email: hoteaioana@yahoo.com
ORCID: https://orcid.org/0000-0003-2552-9835
Affiliation:
1Department of Rheumatology, VieCuri Medical Centre, 5912BL Venlo, The Netherlands
ORCID: https://orcid.org/0000-0003-3700-6257
Affiliation:
1Department of Rheumatology, VieCuri Medical Centre, 5912BL Venlo, The Netherlands
ORCID: https://orcid.org/0000-0003-3026-3154
Explor Musculoskeletal Dis. 2023;1:171–179 DOI: https://doi.org/10.37349/emd.2023.00019
Received: July 14, 2023 Accepted: September 08, 2023 Published: October 30, 2023
Academic Editor: Ivan Castellví Barranco, Hospital Universitari de la Santa Creu i Sant Pau, Spain
Aim: This study aims to analyze the efficacy and safety of benzbromarone as uricosuric, in a real-life clinical setting of a retrospective hospital-based gout cohort.
Methods: Data from gout patients were retrieved from the digital hospital dossiers. Demographics, clinical variables, and laboratory parameters were collected at baseline and 6 months. Efficacy was measured by reaching a serum uric acid (sUA) target < 0.30 mmol/L at 6 months, and the fractional excretion of uric acid (FeUA) was used as a parameter with a potential predictor value.
Results: Data from 98 gout patients were analyzed. Patients were 70 (± 12) years of age, and 90% were male. After 6 months of treatment, 68 out of 98 patients (69%) reached a sUA level < 0.30 mmol/L (5 mg/dL). In patients with a FeUA < 4.5%, so-called low excretors, the FeUA increase was most impressive from 3.2% (± 1.0%) to 12.1% (± 6.9%) after 6 months of benzbromarone treatment (mean increase +8.9% [95% confidence interval (CI): +6.5 to +11.5%], P < 0.001). In non-low excretors, FeUA was on average 7.3% (± 5.1%) and increased to 9.7% (± 6.1%): a mean +2.1% change (95% CI: –2.2 to +6.6%). The increase differed insignificantly in low versus non-low excretors: P > 0.05. Four patients stopped benzbromarone treatment because of a progressive decline in renal function, a condition that was already present before benzbromarone was initiated. Remarkably 38% of patients is still using benzbromarone after 3.8 (± 3.4) years of treatment.
Conclusions: Using the uricosuric benzbromarone in real-life gout patients proved effectivity in lowering sUA levels within 6 months by increasing FeUA significantly. Particularly low excretors benefit from benzbromarone treatment manipulating this mode of action. Determining FeUA in gout patients may further help to find the patient profile benefiting the most from benzbromarone treatment.
A decreased renal urate excretion is the predominant driver of attracting gout, an auto-inflammatory arthritic disease that may develop secondary to hyperuricemia [1, 2]. There is an interest in effective urate-lowering therapies with a uricosuric mode of action. This applies in particular for gout patients in whom urate production inhibitors such as the xanthine oxidase inhibitors (XOi) allopurinol and/or febuxostat are failing or induce side effects [2]. The development of safe uricosurics has been complicated for decades [3] as only benzbromarone and probenecid were approved and selectively marketed in only specific countries [1–3]. During the last decade, novel uricosurics were developed, and specific targets were discovered blocking intrarenal urate transporter 1 (URAT1) and/or organic anion transporter 3 (OAT3) or OAT4 URATs. Pharmaceutics produced drugs manipulating URAT1 aiming to improve benzbromarone: lesinurad [4, 5], verinurad [6], and dotinurad [7]. After a short period of marketing of lesinurad, the latter was withdrawn because of limited selling and safety issues, and the whole uricosuric pipeline appeared a frozen one [8]. Suddenly in 2022, a lack of source material for benzbromarone became a predominant issue, so patients stable while using this drug were left (partially) untreated. We, therefore, wish to learn lessons from our experience within 98 real-life gout patients who had a valid indication for benzbromarone in the Dutch setting with first choice gout therapy for the XOi allopurinol (1st) and febuxostat (2nd). We studied whether calculating a fractional excretion of uric acid (FeUA) may be of value to clinicians using this mode of action therapeutically.
Gout patients diagnosed from 2015 to 2020 were identified in our digital hospital dossiers of the Department of Rheumatology. Data were retrieved from the system and entered anonymously into a CASTOR EDC database (Ioana Hotea). Due to the retrospective and observational approach of the study, a waiver of informed consent was provided. The institutional review board of VieCuri Medical Center, Venlo, Netherlands approved the study. Data were used in agreement with the ethical consent form of the hospital. The inclusion criterium was a diagnosis of gout according to the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD10) code M10. All patients had to be diagnosed based on identifying monosodium urate crystals using polarized light microscopy and/or fulfilling the ACR/EULAR 2015 classification criteria [3].
Patients’ data were collected and stored anonymized on CASTOR for analysis with Statistical Product and Service Solutions (SPSS) version 26. Demographics (age, sex, family history of gout, duration of symptoms, and medication), clinical variables, and laboratory parameters (time frame ± 1 month) at baseline and 6 months were collected. Data outside this time frame were not collected. The definition of comorbidities was based on prespecified diagnoses as available in the digitalized medical record. Renal disease/disorder was added if a patient had an estimated glomerular filtration rate (eGFR) less than 60 mL/min per 1.73 m². Laboratory assessment at baseline and after 6 months included serum uric acid (sUA) and creatinine, eGFR mL/min per 1.73 m². The FeUA was calculated from laboratory assessments of urate and creatinine in blood and urine in the morning void using formula: [(urine urate × serum creatinine)/(sUA × urine creatinine)] × 100.
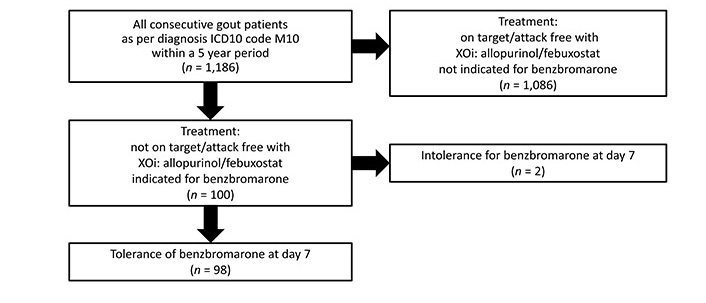
Our electronic database comprised of 1,186 gout patients, all diagnosed within 5 years. We detected 100 patients who were treated to target with an (add-on) uricosuric: benzbromarone 100 mg quaque die (QD) as first choice, if not tolerated, there was a temporary availability of the uricosuric drug lesinurad 200 mg QD second choice. Two patients used lesinurad (due to early intolerance for benzbromarone: severe diarrhea) and 98 patients benzbromarone; the latter group on benzbromarone was included for further analysis into this study, see flow diagram Figure 1 for the design of the inclusion process. The uricosuric treatment was add-on at different time points in the therapeutic process aiming for a treat to target at 6 months.
Patients were 70 (± 12) years of age, and 90% were male. Gout symptoms were reported 8.0 (± 6.5) years before the initial diagnosis. A standard dose of benzbromarone 100 mg QD was prescribed in 81 patients; 70 patients were not on target (< 0.36 mmol/L) using XOi monotherapy and were given an add-on combination therapy with benzbromarone. The baseline characteristics are given in Table 1. Benzbromarone was prescribed during a period of 4.1 (± 5.9) years interquartile range (IQR; 0.04‒9.9) of treatment in 70% of cases in combination with an XOi (allopurinol or febuxostat).
Baseline characteristics of 98 patients indicated for benzbromarone
| Patient characteristics | N (%) |
|---|---|
| Sex | |
| -Male | 8 (90%) |
| -Female | 10 (10%) |
| Duration of symptoms prior to inclusion | |
| -Years (SD) | 8.2 (6.5) |
| Age | |
| -Mean (SD) | 70 (12) |
| Initial dose of benzbromarone | |
| -50 mg QD | 15 (15%) |
| -100 mg QD | 81 (83%) |
| -200 mg QD | 2 (2%) |
| Initial combination therapy | |
| -With allopurinol | 67 (68%) |
| -With febuxostat | 3 (3%) |
| Initial sUA | |
| -Mean (SD), mmol/L | 0.45 (0.12) |
| Initial eGFR | |
| -Mean (SD), mL/min | 54 (18) |
SD: standard deviation
After 6 months of benzbromarone treatment, 68 patients (69%) reached a sUA level < 0.30 mmol/L (5 mg/dL), and 90 out of 98 patients (91%) reached a sUA level < 0.36 mmol/L (6 mg/dL). Patients using the add-on combination therapy versus benzbromarone monotherapy achieved a sUA target < 0.30 mmol/L more frequently: 75.3% versus 64.2%, respectively (P = 0.01) (Figure S1).
The 6-month sUA difference (the initial sUA level and the sUA measuerd at 6 months) achieved with benzbromarone monotherapy (–0.21 mmol/L [95% confidence interval (CI): –0.33 to –0.18]) did not differ from the 6-month sUA difference achieved with combination therapy [–0.23 mmol/L (95% CI: –0.25 to –0.19)]. However, the finally reached sUA levels at 6 months with the XOi-benzbromarone combination therapy were slightly but significantly lower than with benzbromarone in monotherapy: mean difference –0.04 mmol/L, P = 0.02 (95% CI: –0.06 to –0.02).
At the start of benzbromarone, 44 (45%) of patients were known with renal impairment [glomerular filtration rate (GFR) < 60 mL/min]. At 6 months of treatment with benzbromarone, GFR had not changed significantly: mean difference –0.44 mL/min (95% CI: –7.11 to +5.93).
The eGFR in patients using benzbromarone as an add-on with XOi did not change; mean difference in GFR was +0.41 (95% CI: –2.74 to +1.90).
The mean FeUA at baseline was 4.7% (± 3.9%). At 6 months, while using benzbromarone 100 mg QD, the FeUA increased to 10.8% (± 6.4%, P < 0.0001). We found a negative correlation [r = –0.41, P < 0.0001 (n = 92 patients)] between sUA at baseline and GFR at 6 months and between GFR at baseline and sUA at 6 months [r = –0.29, P = 0.004 (n = 92)].
Benzbromarone 100 mg QD was the starting dose in 83% of patients. At 6 months, the following doses were used: 76 patients (77%) used 100 mg QD, 20 patients (20%) used 50 mg QD and two patients used a higher dose of benzbromarone 200 mg QD.
In patients using benzbromarone 50 mg QD, the GFR had slightly but insignificantly decreased: mean of difference –4.8 mL/min, P < 0.7. The FeUA had increased from a mean of 4.4% to 9.5% in 6 months, and the sUA significantly reduced: –0.10 mmol/L (95% CI: –0.22 to +0.01), in combination with a XOi the mean difference even was –0.16 mmol/L (95% CI: –0.27 to –0.05).
Benzbromarone 100 mg QD (in 83% of patients) induced a change in sUA of –0.27 mmol/L (95% CI: –0.34 to –0.19) with an increase of FeUA from 4.7% to 10.9%.
With benzbromarone 200 mg QD the patients registered a decrease in sUA level at 6 months of –0.35 mmol/L (n = 2) and the FeUA at 6 months was 11.3% (n = 2).
In patients using benzbromarone 100 mg QD in combination with XOi, the sUA reduction was –0.23 mmol/L (95% CI: –0.26 to –0.20) from baseline.
The dose of benzbromarone and the initial GFR nor FeUA were correlated. The dose of benzbromarone and sUA at 6 months had a negative correlation: r = –0.21, P = 0.03 (95% CI: –0.40 to –0.01) in 94 patients.
The FeUA was measured at inclusion and after 6 months in 63 (64%) patients. For 35 patients, baseline FeUA was unavailable in the database, so we did not include these patients in the calculation.
Low-excretors (FeUA ≤ 4.5%): At baseline, 36 patients out of 98 (37%) had a low FeUA (FeUA < 4.5%) mean value FeUA 3.2% (± 1.0%). The FeUA increased with the use of benzbromarone on average 3.8 times, mean FeUA value at 6 months was 12.1% (± 6.9%). The FeUA increase on average +8.9% (95% CI: +6.5 to +11.5%), P < 0.001 (Figure S2). Within this group, only three patients did not achieve the sUA target < 0.30 mmol/L and even one patient still had a sUA > 0.36 mmol/L: 92% achieved a sUA < 0.30 mmol/L (5 mg/dL).
Non-low, i.e., normal to high-excretors (FeUA > 4.5%): initially, 27 patients out of 98 (28%) had a FeUA > 4.5%; mean 7.3% (± 5.1%). After 6 months of using benzbromarone, the FeUA had increased to 9.7% (± 6.1%). The FeUA changed on average +2.1% (95% CI: –2.2 to +6.6%), P > 0.05. The respective sUA concentrations were, on average, 0.45 mmol/L and 0.23 mmol/L at the group level at baseline and after 6 months, respectively. Within this non-low excretor group, 70.4 % of patients achieved a sUA < 0.30 mmol/L (5 mg/dL).
FeUA classification: classifying patients into low versus non-low excretors status showed that these groups had a different effect size in response to benzbromarone: FeUA in low excretors significantly increased +8.9% (95% CI: +6.46 to +11.46%); P < 0.0001. FeUA in non-low excretors remained on average unchanged with a +2.1% on average (95% CI: –2.21 to +6.59%).
In low excretor type gout patients (n = 36), a slight improvement of renal function was measured, i.e., GFR +2.2 mL/min (95% CI: –1.49 to 6.06), which is in contrasts with the GFR in non-low excretors (n = 27), i.e., –1.6 mL/min (95% CI: –4.35 to +2.03).
Adverse events were seen more frequently in the non-low, i.e., normal-high excretor group―2 patients developed renal impairment, and 1 case had a liver toxicity issue, compared with the low excretors in whom there were no such reports (Table 2).
Adverse events when using benzbromarone in 98 patients
| Adverse events using benzbromarone | Low excretors (n = 36) | Normal to high excretors (n = 27) | Unknown excretor type at baseline (n = 35) | Total (n = 98) |
|---|---|---|---|---|
| Medical decision to stop benzbromarone | 10 (28%) | 4 (15%) | 4 (11%) | 18 (18%) |
| Renal stones | 0 | 0 | 1 (3%) | 1 (1%) |
| Decreased renal function | 0 | 2 (7%) | 2 (6%) | 4 (4%) |
| Diarrhea | 4 (11%) | 3 (11%) | 2 (6%) | 9 (9%) |
| Patient decision to stop benzbromarone (subjective reasons) | 0 | 5 (18%) | 1 (3%) | 6 (6%) |
| Liver toxicity | 0 | 1 (4%) | 0 | 1 (1%) |
| Ongoing therapy | 13 (36%) | 7 (26%) | 18 (51%) | 38 (38%) |
The data in the table is presented in the form of “n (percentage)”
Benzbromarone 100 mg QD was generally well-tolerated. Adverse reactions were registered though: 9 patients reported diarrhea/frequent stools; in 4 patients, a slight decrease in renal function was seen, and in 1 case, renal stones became symptomatic. The decision to stop the benzbromarone therapy was generally made by the patients, having subjective reasons; a medical decision for quitting benzbromarone therapy was made via a shared decision-making process (the physician and the patient) after completing a debulking period (n = 59). A considerable percentage (38%) still uses benzbromarone therapy: on average, for 3.8 (± 3.4) years.
Benzbromarone was stopped in 4 patients due to decreased GFR; these patients were on uricosuric treatment between 7 months to 72 months. These four patients started benzbromarone with a prior diagnosis of impaired renal function. In this small group, the mean difference in renal function was –14 mL/min (95% CI: –25.8 to –3.69). None of these patients achieved a sUA < 0.30 mmol/L target; interestingly, two were high excretors; FeUA was 8.5 % and 13%, respectively. For the other two, baseline FeUA was not available. They all had a combination with an XOi, and 3 out of 4 were using benzbromarone 100 mg QD.
The main conclusion from this retrospective study comprising 98 patients treated with benzbromarone either in mono- or combination therapy with XOi was that 69% reached the sUA target < 0.30 mmol/L (5 mg/dL) and 91% reached a level < 0.36 mmol/L (6 mg/dL) target irrespective of low or non-low excretor status. Similar results were reported with the selective URAT1 inhibitor dotinurad [4]. In the present study patients with a high sUA level, a low FeUA, and adequate GFR had the best effect size when using this mode of action. In low excretors, FeUA increased by about +9%, whereas in non-low excretors, FeUA excretion remained stable. Only 70% of these non-low excretor-type gout patients achieved the sUA < 0.36 mmol/L target versus 92% of the low excretors. In addition, most side effects were found in the group of patients with a non-low FeUA.
Gout patients can be characterized by clinical manifestations of arthritic attacks with hyperuricemia plus a low urate excretion due to either low GFR or, more specifically, low FeUA [1, 2]. We here demonstrate from a retrospective cohort that subdivision into low versus non-low (normal to high) FeUA status may help clinicians to find the right profile for uricosurics: a low FeUA may increase by factor 4 using a potent uricosuric such as benzbromarone, which enables achieving lower biochemical sUA targets; moreover, the tolerance of benzbromarone appears to be best in these low-excretors. In real life gout patients benzbromarone is stopped either after a period of successful debulking or from late-onset intolerance or adverse events: liver toxicity (1%) and/or loss of renal function (4%) or renal lithiasis (1%). These may well be considered class specific [3–6].
The therapeutic approach in gout, in general, is a dietary limitation of purines and/or urate production inhibitors by XOi, i.e., allopurinol or febuxostat. Their doses are being escalated to reach a predefined clinical and biochemical target [1, 2]. If escalated doses are not tolerated, or targets cannot be achieved, then uricosurics may be considered, i.e., probenecid in the USA and benzbromarone in some European countries including the Netherlands, Spain, Germany, as well as Brazil [2, 3]. Efficacy or safety data from these older drugs come from small studies only. We here showed from an inception cohort that the uricosuric benzbromarone effectively increases urate excretion, particularly in cases with an a priori low FeUA in combination with an adequate renal function. Regarding serious adverse events, we found that using benzbromarone, these side effects occurred in 6% of cases, particularly in patients with an initial higher FeUA from the outset and it hardly occurs in patients with a low excretor status. This may well point to a specific patient profile for optimal efficacy and safety of the potent uricosuric benzbromarone. Further prospective studies powered by GFR and FeUA are needed to find the optimal profile if uricosurics are considered.
Probenecid is a benzoic acid derivative used in gout treatment since 1952 [9, 10]. It is an inhibitor of predominantly urate excretion transporters, the so-called OAT1 and OAT3, a renal tubular transporter facilitating enhanced urate excretion by blocking re-uptake [9–11]. Probenecid is associated with 18% gastrointestinal adverse events, 5% hypersensitivity and rash, and 1 in 3 become intolerant with, therefore, discontinuation of the probenecid. In Europe, probenecid had proven efficacy when suddenly benzbromarone was withdrawn from the market [12, 13]. Benzbromarone is a benzofurane and a potent uricosuric used in gout treatment over the last 30 years but restricted to only a limited number of countries [13]. It inhibits the urate exchanger in the human proximal tubule URAT1, reducing urate reabsorption and potently lowering sUA. Clinical trials showed efficacy (predominantly sUA lowering and reduction of attacks) and safety of benzbromarone [3, 11–16], also in patients with decreased renal function as long as GFR > 20 mL/min, showing effectivity in monotherapy [15, 16], and when in combination therapy with allopurinol or febuxostat [17, 18].
Benzbromarone is considered a potent and safe uricosuric [19]. In our study, serious adverse events were seen more often in patients characterized as non-low, i.e., normal or high excretors, in combination with decreased kidney function. No major safety concerns were raised while using dotinurad, in a small group of patients in Japan [20]. So far, the FeUA has hardly been measured in studies of novel uricosurics, whereas it is the core parameter of their mode of action. We here showed a 3.8-fold increase in FeUA with benzbromarone in low excretors, whereas only 1.3-fold in non-low excretors with about 1 in 3 not achieving the sUA < 0.30 mmol/L (5 mg/dL) as the target. Interestingly, over the last years, European Medicines Agenc (EMA) and Food and Drug Administration (FDA) made lesinurad 200 mg QD available for gout patients irrespective of their FeUA, but lesinurad was withdrawn from the market because of low market penetrance. Lesinurad was an oral selective inhibitor of the renal urate reabsorption transporters URAT1 and OAT4 [5]. Lesinurad 200 mg dose elevated the FeUA 3.6-fold, reduced sUA by about 30% [4], not inhibiting glucose transporter 9 (GLUT9) nor ATP-binding cassette G2 (ABCG2) [5, 21], and showed a low risk for mitochondrial toxicity induction (unlike benzbromarone), and not inhibiting OAT1 nor OAT3 (unlike probenecid). Lesinurad in a monotherapy setting had similar issues as benzbromarone: deterioration of renal function and lithiasis occurring up to 5%-class-specific side effects [6]. In the clinical studies (CLEAR/CRYSTAL), FeUA was not measured for lesinurad, so here we cannot learn whether high excretor status was a predictor for worse outcomes from these studies [22, 23]. The willingness to incorporate FeUA into a study design was recently done in the short-term verinurad study where FeUA was calculated [7]. Another study using FeUA for classifying gout patients as underexcretors showed a 60% success rate of benzbromarone in achieving a target sUA level < 0.36 mmol/L [24]. Lesinurad monotherapy 400 mg and 600 mg QD demonstrated class-specific renal side effects in about 5–10% [21] and verinurad showed these in 11.6%. Whether these are associated with higher FeUA status is unclear as these data were not provided. In future studies, it may be crucial for all patients in studies to complete a full urate profile metabolism, including FeUA prior and after uricosuric therapy. This may indicate towards a specific group of patients who can benefit the most from this specific medication and at the same time may help prevent renal side effects.
In conclusions, we learned from retrospective benzbromarone data that efficacy and safety are best if prescribed in low excretor gout patients, with over 90% achieving a 0.30 mmol/L sUA target. If targets cannot be reached in gout patients, an add-on uricosuric may be considered, particularly in low excretors.
CI: confidence interval
eGFR: estimated glomerular filtration rate
FeUA: fractional excretion of uric acid
GFR: glomerular filtration rate
OAT3: organic anion transporter 3
QD: quaque die
sUA: serum uric acid
URAT1: urate transporter 1
XOi: xanthine oxidase inhibitors
The supplementary material for this article is available at: https://www.explorationpub.com/uploads/Article/file/100719_sup_1.pdf.
IH: Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing—original draft, Writing—review & editing. MJ: Methodology, Resources, Validation, Writing—review & editing. TLJ: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing—review & editing. All authors read and approved the submitted version.
The authors declare that they have no conflicts of interest.
The institutional review board of VieCuri Medical Center (2021-009), Venlo, Netherlands approved the study.
Due to the retrospective and observational approach of the study a waiver of informed consent was provided.
Not applicable.
Not applicable.
IH was supported by
© The Author(s) 2023.
Copyright: © The Author(s) 2023. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.

View: 8856
Download: 25
Times Cited: 0