Systematic Review
Systematic Review

Affiliation:
1Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Tarsus University, Mersin 33400, Türkiye
Email: alimutlu708@gmail.com
ORCID: https://orcid.org/0000-0001-9182-394X
Affiliation:
2Faculty of Medicine, Kirsehir Ahi Evran University, Kırşehir 40100, Türkiye
ORCID: https://orcid.org/0000-0003-4670-4794
Affiliation:
3Department of Physiotherapy and Rehabilitation, School of Physical Therapy and Rehabilitation, Kirsehir Ahi Evran University, Kırşehir 40100, Türkiye
ORCID: https://orcid.org/0000-0002-1163-9972
Affiliation:
3Department of Physiotherapy and Rehabilitation, School of Physical Therapy and Rehabilitation, Kirsehir Ahi Evran University, Kırşehir 40100, Türkiye
ORCID: https://orcid.org/0000-0001-5898-1698
Explor Neuroprot Ther. 2023;3:470–480 DOI: https://doi.org/10.37349/ent.2023.00063
Received: May 10, 2023 Accepted: November 14, 2023 Published: December 26, 2023
Academic Editor: Noureddin Nakhostin Ansari, Tehran University of Medical Sciences, Iran
The article belongs to the special issue Dry Needling for Neurological Disorders
Aim: The aim of this study is to review the effectiveness of dry needling in patients with multiple sclerosis (MS).
Methods: PubMed, Physiotherapy Evidence Database (PEDro), Web of Science, Scopus, and Cochrane Library databases were searched from its inception until July 2023 and the reference lists of the articles obtained were manually searched. Studies examining the effectiveness of dry needling treatment alone or in combination with a different protocol in individuals diagnosed with MS, regardless of type, were included. The systematic review included quasi-experimental studies and case reports. Studies involving traditional Chinese medicine acupuncture applications, conference abstracts, and protocol records were excluded. Methodological quality assessments were carried out independently by two authors using tools developed by the Joanna Briggs Institute (JBI).
Results: A total of 130 studies were found in the searches. Some studies were excluded due to duplication, protocol registration, conference abstract, and content outside the scope of the study and 7 studies were included in the review. In total, 33 individuals were included in this review, 22 of whom were women. Four studies specified the MS type of the patients, while the other studies did not specify MS type.
Conclusions: Despite some limitations, this is, to our knowledge, the first review summarizing studies evaluating the effectiveness of dry needling in MS patients. The dry needling technique alone or in a combination of treatments was effective in improving pain, spasticity, range of motion, dexterity, mobility, limb function, and quality of life in MS patients. However, these results should be treated with caution due to the small number of included studies and the lack of randomized controlled trials. Although it is too early to talk about the positive effects of the dry needling technique in MS patients, the study results are promising. More randomized controlled trials should be conducted on this topic.
Multiple sclerosis (MS) is a chronic autoimmune inflammatory disease of the central nervous system. Young adults and women are at higher risk, it is clinically characterized by involvement of mostly motor, sensory, visual, and autonomic systems and results in progressive loss of function [1, 2]. MS is one of the most common neurological disorders in the world, its incidence and prevalence are increasing in both developed and developing countries, and the underlying causes of the disease remain unclear [3]. There is no definitive cure for MS. The treatment process is shaped in line with the goals of improving symptoms, controlling dysfunctions characterized by disease progression, and preventing attacks [4]. Common symptoms of the disease include fatigue, partial or complete paralysis of the lower and upper extremities, spasticity, gait and balance disorders, bladder and bowel problems, visual disturbances, cognitive impairments, and depression [5].
Dry needling is a treatment approach commonly applied to myofascial trigger points for the treatment of muscle pain in musculoskeletal diseases [6, 7]. In recent years, studies have shown the positive effects of dry needling on improving spasticity, pain, gait, postural control, and function in various neurological diseases such as stroke [8–12], spinal cord injuries [13], brain tumors [14], Parkinson disease [15]. It is known that disability caused by neurological diseases leads to an increase in costs, either directly or indirectly; studies in patients with stroke have shown that dry needling is cost-effective, and in this respect, it can be said that it is a worthy of further investigation [16–18].
Dry needling is a relatively new approach that is not yet widely used in patients with MS. The acupuncture technique, which has a longer history in the treatment of MS, can be seen as similar applications to dry needling. There are significant differences between these two applications using very similar needles. In the acupuncture approach, applications are made for “meridians”, while in dry needling, applications can be made for muscles, ligaments, scar tissues, and peripheral nerves [19]. In the literature, there is a review examining acupuncture applications according to the traditional Chinese medical approach in patients with MS [20], but there is no review study examining the use of the dry needling technique in MS patients. The study aims to review the studies examining the effectiveness of dry-needling applications in MS.
This study was carried out as a systematic review. Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) were followed in the creation of the study protocol and writing the report [21].
The search strategy includes five electronic databases from its inception until July 2023, and these databases are: PubMed, Physiotherapy Evidence Database (PEDro), Web of Science, Scopus, and Cochrane Library. The following search terms were used in the literature search, which was created with the terms MS and dry needling in mind: [(“dry needle” OR “needling”) AND (“multiple sclerosis” OR “disseminated sclerosis” OR “MS”)]. All databases except PEDro were searched using these search terms. Since the use of boolean conjunctions is limited in the PEDro database, the following search term combinations were used during the search: “needling” AND “MS”, “dry needle” AND “MS”, “dry needle” AND “multiple sclerosis”, “needling” AND “multiple sclerosis”, “needling” AND “disseminated sclerosis”, “dry needle” AND “disseminated sclerosis”. The databases were searched using the following methods and no limitations were used during these searches: PubMed, all fields search; PEDro, simple search and only trial studies were included; Web of Science, topic search; Scopus, article title abstract keywords search; Cochrane Library, title abstract keyword search and only trial studies were included.
Studies examining the effectiveness of dry needling treatment alone or in combination with a different protocol in individuals diagnosed with MS, regardless of type, were included. The systematic review included quasi-experimental studies and case reports. Studies involving traditional Chinese medicine acupuncture applications, conference abstracts, and protocol records were excluded.
All studies obtained after the literature search were independently evaluated by two authors (AM and MHK) using Zotero (version 6.0.26). After removing duplicate studies, both authors independently screened all studies by title and abstract, and irrelevant studies were excluded. The full texts of the obtained studies were evaluated by the authors considering the inclusion and exclusion criteria, and the results were combined by the authors in a joint meeting. Any disagreements were resolved in a joint meeting involving a third author (ÖB). The reference list of the studies whose full text was evaluated was also scanned by the authors.
Methodological quality assessments of the studies included in this systematic review were performed independently by two authors (AM, MHK) and the results were combined by the authors in a joint meeting. Any disagreements were resolved at a joint meeting involving a third author (ÖB). Quality assessments of the included studies were made using the 2020 versions of the “Checklist for Quasi-Experimental Studies (Non-Randomized Experimental Studies)” [22] and “Checklist for Case Reports”[23] tools developed by the Joanna Briggs Institute (JBI). The checklist contains 9 questions for quasi-experimental studies, and 8 questions for case reports. The responses to the questions are in the form of “Yes,” “No,” “Unsure,” and “Not applicable.”
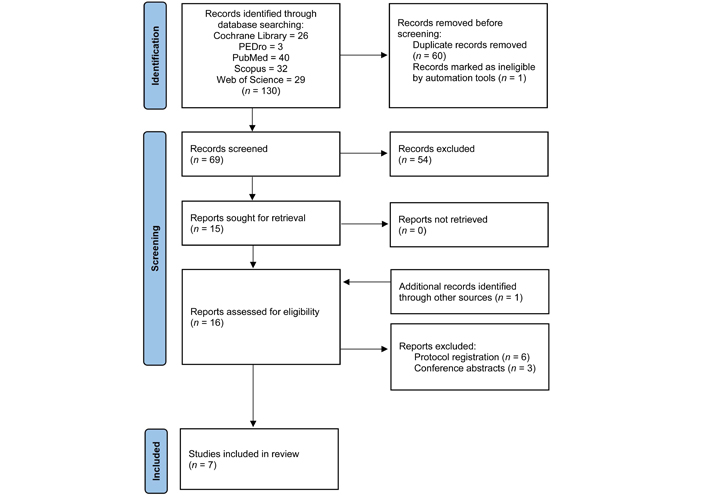
A total of 130 studies were found as a result of the search. Sixty of the studies were eliminated due to duplication and one study was eliminated due to withdrawal of the study. As a result of the title and abstract analysis, 15 studies were obtained for full-text evaluation. A suitable study from the reference list of a study that was not included in this systematic review because it was a protocol record was included in this systematic review. In total, the full text of 16 studies was evaluated and 9 inappropriate studies were excluded as a result of the evaluations. The flow diagram in Figure 1 shows the article selection procedure, according to PRISMA guidelines.
In total, 33 individuals were included in this review, 22 of whom were women. Four studies specified the MS type of the patients [24–27], while the other studies did not specify MS type. The results of the studies are summarized in Table 1 (study purpose, design and subjects) and Table 2 (interventions, findings, conclusions and comments).
Study purpose, design and subjects
| Study | Purpose | Design | Subjects |
|---|---|---|---|
| McDowell et al., 2015 [28] | To investigate fecal incontinence in a patient with MS receiving dry needle therapy | Case report | n = 1, 57-year-old female patient with MS diagnosed in 1981 |
| Miller et al., 2022 [27] | To investigate the effect of a combination of intramuscular electrical stimulation using the dry needles and treadmill therapy supplemented with functional electrical stimulation on gait, spasticity, fatigue and muscle strength | Pretest–posttest quasi-experimental design | n = 16, mean age = 47.9 ± 10, diagnosed with relapsing remitting, primary progressive or secondary progressive MS |
| Luque-Moreno et al., 2020 [26] | To investigate the effects of deep dry needling technique on spasticity, pain and range of motion (ROM) in a patient with secondary progressive MS | Case report | n = 1, 35-year-old female patient was diagnosed as relapsing remitting in 2009 and transformed into secondary progressive form in 2013, expanded disability status scale (EDSS) score = 6.5 |
| Khalifeloo et al., 2022 [29] | To investigate the immediate effects of dry needling on spasticity and mobility in a female patient with MS | Case report | n = 1, 38-year-old female patient treated for MS for 4 years, EDSS Score = 5.5 |
| Javier-Ormazábal et al., 2023 [25] | To investigate the effect of ultrasound-guided percutaneous neuromodulation on grip strength and hand function | Case report | n = 1, 51-year-old male patient diagnosed with MS in 2007 |
| Del Pilar Pérez-Trujillo et al., 2021 [24] | To examine the effectiveness of dry needling in the treatment of spasticity in MS patients | Pretest–posttest quasi-experimental design | n = 12, 3 males, mean disease age = 13 years, patients with EDSS scores higher than 2.5 |
| León et al., 2023 [30] | To evaluate the effect of dry needling on spasticity measured by the rate-dependent depression (RDD) of the Hoffman (H) reflex in an MS Patient | Case report | n = 1, 48-year-old male with MS for 25-year |
Interventions, findings, conclusions and comments
| Study | Intervention | Outcome measures | Results | Conclusion/Comments |
|---|---|---|---|---|
| McDowell et al., 2015 [28] | Dry needling at the L4 level to the multifidus; gluteus maximus, gluteus medius and gluteus minimus; right upper trapezius muscle | Subjective reports of fecal incontinence, lower limb heaviness and increased fatigue | After dry needling treatment, fecal incontinence seizure and a feeling that starts as a “cotton wool” feeling in the legs and turns into a “heavy leg” | It describes fecal incontinence, lower limb heaviness and increased fatigue shortly after dry needling was performed in a patient with MS and emphasizes that special care should be taken in the treatment of dry needling in these patients with MS |
| Miller et al., 2022 [27] | 2 days a week for 12 weeks, 1–4 weeks intramuscular electrical stimulation to the medial and lateral heads of the gastrosoleus followed by functional electrical stimulation assisted treadmill treatment combination application, 5–12 weeks only functional electrical stimulation assisted treadmill treatment combination application | Timed 25-foot walk (T25FW), 6-minute walk test (6MWT), Berg balance scale (BBS), Modified Ashworth Scale (MAS), 10-second foot tap test, heel raises until fatigue, modified fatigue impact scale (MFIS) | Significant increase in 6MWT results, significant decrease in T25FW results, significant increase in the number of heel raises to exhaustion, significant decrease in MAS, improvement in fatigue levels measured by MFIS in (56%) of participants | The applied treatment combination has the potential to reduce spasticity and increase walking speed and endurance in patients with MS |
| Luque-Moreno et al., 2020 [26] | Once a week for 2 weeks, dry needling with the “fast in fast out” technique on the midpoint of the muscle body of the rectus femoris and gastrocnemius medialis until at least 3–4 local twitch responses are obtained | Visual analog scale (VAS), algometer, MAS, ROM, 2MWT, MS international quality of life questionnaire (MusiQoL) | Decrease in pain in the rectus femoris muscle according to VAS, increase in pain tolerance in the gastrocnemius medialis muscle and decrease in the rectus femoris muscle in algometer measurements, decrease in spasticity in both muscles according to the MAS, improvement in gait speed, increase in quality of life score | The authors imply a functional improvement in walking even in the case of progressive disease, but changes in perceived pain and ROM are not conclusive. Continued research in this area is needed to obtain more evidence |
| Khalifeloo et al., 2022 [29] | Single session of 1 min dry needling application to the long head of the biceps femoris muscle and semitendinosus muscle using the “fast in fast out” technique | T25FW, MAS, hamstring stiffness | A 43% improvement in the T25FW, a 31% decrease in muscle stiffness and a reduction in spasticity for both muscles | It shows that treatment using dry needling has a positive effect on spastic muscles and improves mobility in this patient with MS. Further research is needed to evaluate the effects of dry needling in MS patients with spasticity |
| Javier-Ormazábal et al., 2023 [25] | Single session, ultrasound-guided percutaneous neuromodulation with dry needling on the median nerve between the two heads of the pronator teres muscle | 9-hole peg test (9HPT), grip strength measured with a dynamometer | A significant increase in grip strength immediately after treatment and a gradual increase at day 1 and day 4 follow-up, improvement in hand function immediately after treatment and this improvement was maintained at 4-day follow-up | It shows that a single session of ultrasound-guided percutaneous neuromodulation may be effective to improve hand function and grip strength in a patient with MS. The application of dry needling and percutaneous neuromodulation in patients with neurological impairment should be investigated with larger samples and randomized controlled trials |
| Del Pilar Pérez-Trujillo et al., 2021 [24] | Dry needling only on the lower extremities (muscles not specified) for 4 months, 3 times a month | The Penn spasm frequency scale (PSFS), VAS of spasticity, EDSS score, The timed-up and go (TUG) test, T25FW, 9HPT, multiple sclerosis quality of life-54 (MSQoL-54) | Reduction in spasticity in the lower extremities in treated muscles, improvement in upper extremity function despite no treatment, improvement in EDSS score, improvement in T25FW and TUG test, improvement in PSFS and VAS scores, improvement in quality of life (Significant changes disappeared in all tests one month after treatment) | Dry needling in patients with MS is reported to contribute to improvements in spasticity, upper limb function, mobility, pain and quality of life, but the effect is not permanent. A larger sample is needed to predict long-term outcomes in MS patients and to validate the application of the technique |
| León et al., 2023 [30] | The protocol consisted of seven dry needling sessions, once per week. Dry needling was performed bilaterally in the vastus lateralis, vastus medialis, biceps femoris, and semitendinosus muscles | Baseline data of the RDD of the H reflex, 10MWT, and the 6MWT were evaluated in the first session before dry needling | Results suggest a partial reduction in spasticity represented by decrease of the excitability of the neural elements involved in the RDD of the H reflex following dry needling. Walking distance is increased at 6MWT | The RDD of the H reflex could be used as a biomarker of spasticity. A larger sample is warranted for evaluating the RDD of the H reflex to study central and peripheral nervous mechanisms of dry needling on spasticity |
The quality assessment scores for the quasi-experimental studies were yes: 7/9 in 2 studies. The quality assessment scores for the case reports were yes: 7/8 in 4 studies and 8/8 in another study (Table 3).
Quality assessment results of the studies
| Study | JBI critical appraisal checklist | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Quality | |
| Quasi-experimental studies | ||||||||||
| Miller et al., 2022 [27] | Y | Y | N | N | Y | Y | Y | Y | Y | Y 7/9 |
| Del Pilar Pérez-Trujillo et al., 2021 [24] | Y | Y | N | N | Y | Y | Y | Y | Y | Y 7/9 |
| Case reports | ||||||||||
| McDowell et al., 2015 [28] | Y | Y | Y | Y | Y | Y | Y | Y | Y 8/8 | |
| Luque-Moreno et al., 2020 [26] | Y | Y | Y | Y | Y | Y | N | Y | Y 7/8 | |
| Khalifeloo et al., 2022 [29] | Y | Y | Y | Y | Y | Y | N | Y | Y 7/8 | |
| Javier-Ormazábal et al., 2023 [25] | Y | Y | Y | Y | Y | Y | N | Y | Y 7/8 | |
| León et al., 2023 [30] | Y | Y | Y | Y | Y | Y | N | Y | Y 7/8 | |
Y: Yes; N: No
The dry needling techniques applied in the studies varied. Two studies used the “fast in-fast out” technique [26, 29, 30], one study used the “sparrow pecking” technique [28], one study used the intramuscular electrical stimulation technique [27], one study used the neuromodulation technique [25], and in one study no detailed information was given about the dry needling technique [24].
Pain was evaluated in three studies. Luque-Moreno et al. [26] evaluated pain with VAS before, after and during treatment and also evaluated pressure pain threshold with algometer before and after treatment. After treatment, there was a 2 point decrease in pain in the rectus femoris muscle according to VAS, an increase in pain tolerance in the gastrocnemius medialis muscle and a decrease in the rectus femoris muscle in algometer measurements. During the treatment, pain according to VAS was 8 points in the rectus femoris muscle and 2 points in the gastrocnemius muscle. In the study by McDowell et al. [28], the patient’s overall pain score was 6/10 according to the Numerical Pain Rating Score before treatment. The treatment was terminated due to side effects and no information about the pain score was provided at the end of the treatment. Pain assessed with VAS by Del Pilar Pérez-Trujillo et al. [24] decreased significantly (P = 0.009) in all participants after treatment. One month after the end of treatment, the decrease in pain score was not statistically significant, although it was maintained.
ROM was evaluated in two studies. Luque-Moreno et al. [26] evaluated passive ROM of ankle dorsiflexion, knee flexion, hip flexion and extension using a goniometer before and after treatment and found no change except an eight-degree increase in hip extension. McDowell et al. [28] reported that the patient’s lumbar spine ROM was 25% less before treatment. The treatment was discontinued due to side effects and no information on ROM was provided at the end of treatment.
Fatigue was evaluated in two studies. Although fatigue was not evaluated in the study by McDowell et al. [28], the patient reported that there was a feeling of “cotton wool” in his legs after the treatment and this sensation continued for 24 h and turned into a feeling of “heavy leg” below his knees and his general fatigue increased. Miller et al. [27] used the MFIS to assess fatigue in their study. Nine out of sixteen participants (56%) reported improvement in fatigue levels measured by MFIS.
Quality of life was evaluated in two studies. Luque-Moreno et al. [26] assessed quality of life with MusiQoL before and after treatment and showed improvement in quality of life. Del Pilar Pérez-Trujillo et al. [24] assessed quality of life with the MSQoL-54 before and after treatment and found improvements in quality of life. One month after the end of treatment, improvements in quality of life were maintained, but not statistically significant.
Spasticity was evaluated in five studies. Luque-Moreno et al. [26] evaluated spasticity in the rectus femoris and gastrocnemius medialis muscles before and after treatment with the MAS and found a decrease in spasticity. Khalifeloo et al. [29] evaluated spasticity in the quadriceps femoris and hamstring muscles before and after treatment with the MAS and found a decrease in spasticity. Miller et al. [27] evaluated spasticity in the lower extremities before and after treatment with the MAS. A significant decrease in spasticity (P = 0.004) was observed between the 1st–4th sessions of intramuscular electrical stimulation and a significant decrease in spasticity (P = 0.0005) was found between the 1st-12th sessions, which refers to the beginning and end of treatment. Del Pilar Pérez-Trujillo et al. [24] evaluated spasticity in the lower extremities before and after treatment with the PSFS and found a significant decrease in spasticity (P = 0.017). León et al. [30] reported a partial reduction in spasticity represented by decrease of the excitability of the neural elements involved in the RDD of the H reflex following dry needling.
Mobility was evaluated in five studies. Luque-Moreno et al. [26] evaluated mobility with the 2MWT and the GaitRite gait analysis system before and after treatment. Improvement in walking speed was observed, cadence did not change, walking speed increased by 5 cm/s in the 2MWT, but it was not clinically significant. McDowell et al. [28] reported a 100-meter walk score of 9/10 according to the patient specific functional scales before treatment. The treatment was terminated due to side effects and no information about mobility was given at the end of treatment. Khalifeloo et al. [29] evaluated mobility with the T25FW before and after treatment. At the end of treatment, the time to complete the test decreased from 16.3 seconds to 9.29 seconds, indicating a 43% improvement. Miller et al. [27] assessed mobility with the T25FW and the 6MWT before and after treatment. As a result of these evaluations, an increase in walking distance and walking speed was found. Del Pilar Pérez-Trujillo et al. [24] evaluated mobility before and after treatment with the T25FW and TUG test. The results of these tests showed significant improvements (P = 0.016 and P = 0.016, respectively). León et al. [30] evaluated mobility with the 6MWT before and after treatment. They reported walking distance is increased at 6MWT.
Dexterity was evaluated in two studies and grip strength in one study. Javier-Ormazábal et al. [25] evaluated dexterity with a 9HPT and grip strength with a dynamometer. The evaluations were performed before treatment, immediately after treatment, 1 day after treatment and 4 days after treatment. There was a significant improvement in grip strength immediately after treatment and this improvement gradually increased on day 1 and day 4 follow-up. Improvement in hand function was seen immediately after treatment and this improvement was maintained at 4-day follow-up. Del Pilar Pérez-Trujillo et al. [24] evaluated dexterity with the 9HPT before and after treatment. In the study, significant improvements in fine motor skills were found as a result of decreased spasticity in the upper extremity, although no intervention was performed in the upper extremity. Improvement in upper extremity functions despite treatment of the lower extremity should be investigated in future studies.
Although positive effects of dry needling applications have been observed in MS, limitations in the studies on the topic should not be ignored. Inadequate sample size, short treatment durations, lack of randomization and control group are some of them. In addition, the majority of the studies consisted of case reports and therefore advanced statistical analyses could not be performed. This reduces the reliability of the studies. Nevertheless, these studies show promise in improving pain, spasticity, ROM, dexterity, mobility, limb function and quality of life in MS patients.
There are few protocol registration in the literature with study designs that include control groups, blinding, and randomization addressing dry needling in MS [31, 32], but these studies have not yet been concluded. This topic should be investigated more reliably with randomized controlled trials in the future.
In the included studies, the dry needling technique was mostly applied alone, but some studies included intramuscular electrical stimulation. In order to compare the results of the studies and evaluate the effect of dry needling in MS patients, it is important to provide detailed information about the dry needling technique and the participants, and to indicate whether any other treatment was used in combination with dry needling.
EDSS score is important to assess the severity of the disease and functional status in MS patients [33]. In half of the studies included in the review, the EDSS score was ignored. This makes it difficult to determine the patient groups in which dry needling can be applied. Fatigue is one of the symptoms that greatly affect the quality of life in MS. Fatigue symptom was not evaluated in the majority of the studies.
Only one of the included studies showed that dry needling caused adverse effects in patients with MS, and the adverse effects disappeared with the termination of treatment [28]. Although the authors could not fully explain the cause of this adverse effect, the short duration of the adverse effect and the fact that no adverse effects were mentioned in other studies suggest that dry needling may be safe in patients with MS.
Despite some limitations, to the best of our knowledge, this is the first review summarizing studies evaluating the effectiveness of dry needling in MS patients. One of the most important limitations is that most of the included studies are case studies due to the lack of literature. Following the development of the literature on this topic, well-designed systematic reviews and meta-analyses are needed.
In conclusion, the dry needling technique has been effective in improving MS symptoms (pain, spasticity, ROM, dexterity, mobility, limb function and quality of life) alone or in a combination of treatments. However, these results should be treated with caution due to the small number of included studies and the lack of randomized controlled trials. Although it is too early to talk about the positive effects of the dry needling technique in MS patients, the study results are promising. More randomized controlled trials should be conducted on this topic.
6MWT: 6-minute walk test
9HPT: 9-hole peg test
EDSS: expanded disability status scale
H reflex: Hoffman reflex
MAS: Modified Ashworth Scale
MFIS: Modified Fatigue Impact Scale
MS: multiple sclerosis
PEDro: Physiotherapy Evidence Database
PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses
PSFS: the Penn spasm frequency scale
RDD: rate-dependent depression
ROM: range of motion
T25FW: timed 25-foot walk
TUG test: the timed-up and go test
VAS: visual analog scale
AM: Conceptualization, Investigation, Methodology, Validation, Writing—original draft, Writing—review & editing. MHK: Investigation, Methodology, Validation, Writing—review & editing. ÖB: Conceptualization, Methodology, Supervision, Writing—original draft, Writing—review & editing. BB: Methodology, Supervision, Writing—original draft.
The authors declare that they have no conflicts of interest.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
Not applicable.
© The Author(s) 2023.
Copyright: © The Author(s) 2023. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Nirmal Surya, Guhan Ramamurthy
Seyedeh Saeideh Babazadeh-Zavieh ... Korosh Mansoori
Daniel Fernández ... Eva María Gómez-Trullén
Temrah Okonski, Jan Dommerholt