
Abstract
Aim:
Forward head posture (FHP) is a very common pathological neck posture among people who frequently use multimedia devices, and it could be related to some musculoskeletal disorders. However, its role in influencing lung function and its relationship with neck disability are still debated in the literature. Therefore, the aim of the present study was to investigate the influence of FHP on respiratory function, and to explore a possible relationship between FHP and neck discomfort.
Methods:
A cross-sectional study was conducted on a sample of 83 subjects (35.7 ± 8.4 years aged), enrolled at the Ferrari corporate wellness program “Formula Benessere”. Craniovertebral angle (CVA) was measured with a digital goniometer to assess head posture: FHP was defined with a CVA < 50° in an upright position. Spirometry was conducted according to European Respiratory Society/American Thoracic Society (ERS/ATS) criteria. Finally, subjects enrolled were evaluated through a self-administered neck disability index (NDI) questionnaire.
Results:
Among the 60 participants with agreement about the CVA measurements, 45 had FHP (11 females and 34 males) with lower CVA values. No significant differences were found in spirometric parameters between subjects with FHP (n = 45) and subjects without FHP (n = 15). Furthermore, the two groups did not differ either in NDI scores (P = 0.148).
Conclusions:
There is no clear relationship between FHP and respiratory function indices. Moreover, no differences have been found in NDI values between subjects with FHP and subjects without FHP. Respiratory rehabilitation strategies should be focused on other parameters than FHP itself.
Keywords
Forward head posture, neck posture, spirometry, peak expiratory flow, neck disability index, chronic neck painIntroduction
Forward head posture (FHP) is a particular posture of neck, caused by the hyperextension of the upper cervical vertebrae and its forward translation [1]. The National Academy of Sports Medicine defines FHP as a forward-tilted positioning of head, out of the neutral alignment (neutral head posture—NHP).
This condition is relatively common in several jobs involving long-term static postures and the use of multimedia devices, especially smartphones and computers [2]. It can lead to a painful shortening of the muscles of the back of the neck, causing muscle imbalances due to an abnormal cervical muscle load; moreover, it increases the compressive forces on the articular facets and the inter-vertebral ligaments [1, 3]. Subjects with FHP often have a significant reduction of the cervical spine range of motion (ROM), and a higher incidence of dorsal kyphosis. As a result, pain is a possible outcome in some of these subjects [3–5], even if there is not a clear association between FHP and neck pain, headache, temporomandibular arthralgia and musculoskeletal disorders [6].
Several studies reported a significant influence of FHP on respiratory function, determined by a general weakening of the accessory respiratory muscles [7–9]. The FHP role in respiratory function was found to be more pronounced in patients already suffering from chronic respiratory diseases [10], with a reduction of forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1) and the activity of the accessory muscles of respiration [11]. It has been hypothesized that the observed alterations in respiratory function may arise from morphological changes in the thoracic shape and from the limited mobility of the last thoracic ribs during inspiration [12]. Koseki et al. [13] analyzed the thoracic conformation and chest movements during inspiration and expiration of 15 healthy males, reporting a significant anterior transposition of the upper chest both at rest and during maximal inspiration in subjects with FHP compared to those with NHP.
As a result, subjects with FHP are often directed towards a respiratory rehabilitation pathway.
Moreover, the influence of neck pain on the strength of the respiratory muscles should not be underestimated, as it has been found that subjects with FHP suffering from chronic neck pain have a lower level of respiratory muscle strength [14] and a shortening of the accessory respiratory muscles. This accessory muscle deterioration has a great impact on their effectiveness in supporting the respiratory function [15].
Since the literature on the topic is not particularly explanatory, and considering the high prevalence of postural problems and neck pain in the general population, the aim of this study was to investigate the influence of FHP on respiratory function, and secondly to explore a possible relationship between FHP and neck discomfort.
Materials and methods
Study design, ethics, settings
The study was carried out during the annual “Ferrari Formula Benessere” program, a corporate wellness program implemented by Ferrari S.p.A. car company, dedicated to employees of the Ferrari group and their families. Med-Ex is the private society that managed it [16]. This project provides periodic check-ups on an annual basis, based on physical efficiency tests, detection of anthropometric and bioimpedance parameters and a complete medical examination. The effectiveness of this corporate wellness project has already been proved [17, 18].
All participants gave written, informed consent. Adhesion to “Ferrari Formula Benessere” program was totally free and based on personal voluntary agreement. Before the visit, each patient signed an informed consent accepting medical procedures and data collection by Med-Ex. Moreover, the data-collection form specified that data would be used for scientific purposes, in aggregate form and the privacy of each specific subject would be maintained. Med-Ex treated the data according to privacy and protection policies. Personal and medical subjects’ data were collected through a pre-designed original medical database. All clinical data assembled from individuals are kept in the institution database and individual privacy was fully respected. The study was carried out in accordance with the principles of the Declaration of Helsinki.
Participants
This study involved a heterogeneous and convenience sample. The subjects were selected among those at the first entrance of the “Ferrari Formula Benessere” program, between October and December 2021. We included male and female subjects aged more than 18 years, and exclusion criteria were: a) smoking habits; b) known chronic respiratory diseases; c) occupational exposure to dust and volatile substances; d) spine or thoracic surgery; e) primary or acquired deformities of the thoracic cage; f) previous thoraco-mediastinal irradiation for proliferative pathologies; g) all sorts of spinal pain.
The first outcome of the study was to evaluate if subjects with FHP had an abnormal spirometry; the second outcome was to assess if subjects with FHP tested positive at neck disability index (NDI) questionnaire.
Head posture assessment
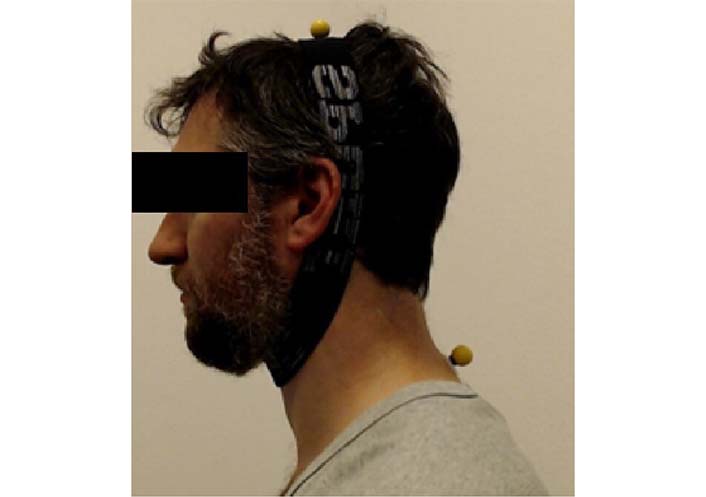
All measurements were performed by the same experienced physical trainer. For the acquisition, adhesive marks were fixed at the spinous apophysis of the seventh cervical vertebra (C7) and at the vertex point of the head (vertex) of the subjects using an elastic band (Figure 1). The photographs were taken on the left and right profile with the subjects’ neck in a neutral position (NHP) and then in a position of maximum extension and flexion, in order to calculate the craniovertebral angle (CVA) during post processing. NHP was defined as a relaxed head position with the head maintained in the vertical position [1]. To assess head posture, we measured the CVA with the aid of a digital goniometer (GeoGeBra software). The CVA is represented by the intersection of the horizontal line passing through the spinous process of the C7, with a line that joins the midpoint of the tragus of the auricle to the spinous process of C7 [1] (Figure 2). The posture of the head is commonly defined as FHP when the CVA is less than 50° in an upright position [3, 4].
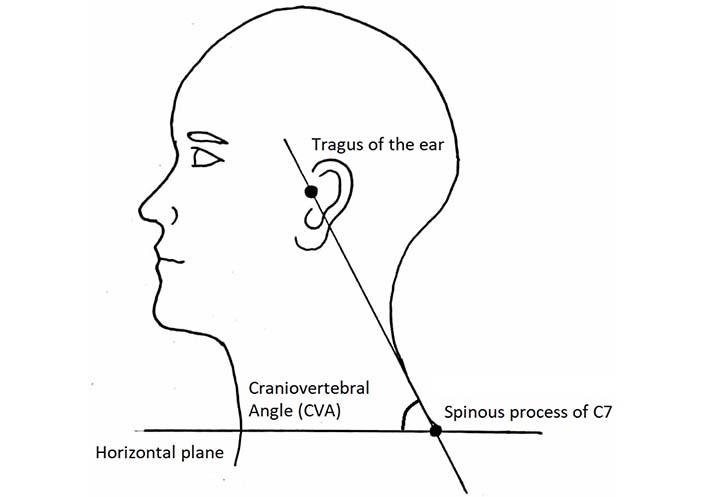
Subsequently, with the aid of a digital goniometer, each participant’s CVA was measured using the method described by Grimmer-Somers et al. [19], and therefore by measuring the acute angle between the line joining C7 to the tragus of the ear and the horizontal line at C7.
Spirometry
The spirometry exam was performed in a sitting position and subjects used a nose clip to keep the nostrils closed. Spirometry was completed using a COSMED microQuark Spirometer that was calibrated prior to each testing session. All measurements were performed by the same experienced sport medicine physician. Testing parameters included FVC, FEV1, peak expiratory flow (PEF), maximal expiratory flow (MEF)25/50/75, forced expiratory volume in six seconds (FEF), VC, inspiratory capacity (IC), maximum voluntary ventilation (MVV). We accepted for our study only spirometry of at least grade C of quality. We used the Report of the Global Lung Function Initiative (GLI) as reference for cut-off values [20]. Each subject normally performed 3 “acceptable” FVC evaluation tests according to the European Respiratory Society/American Thoracic Society (ERS/ATS) criteria [21], in order to have repeatable results and to obtain 3 acceptable spirograms in which FEV1and FVC differ no more than 200 mL or 5% and for PEF no more than 10%: the best result was recorded for each value [21].
Neck disability index
The subjects enrolled were evaluated through a self-administered NDI questionnaire, to investigate the existence and degree of disability of the cervical spine [6]. Currently, the NDI is the most used tool to assess cervical disability in subjects with neck pain, with the aim of quantifying the disability and subsequently the effectiveness of the therapeutic intervention [7, 8]. The NDI score is the sum of different items, and the higher the score, the greater the dysfunction related to abnormalities around the neck.
Statistical analysis
All statistical analyses were performed using SPSS (version 25.0, IBM Corp., USA). Mean, median and standard deviation (SD) were used as distribution indices. For normality test, Shapiro-Wilk test was used. Independent t-test was used to compare the difference between the FHP group and the non-FHP group. All statistical significance levels (α) were set to 0.05.
Results
Eighty-three subjects (16 females, 67 males), with an average age of 35.69 ± 8.39 years (median 33 years) were analyzed. The value of the CVA, measured on the left side was on average 45.54° ± 5.74° (median 45.73°), while on the right was 48.74° ± 6.01°, (median 49.17°).
We determined that there was agreement between right and left CVA when the values differed by no more than 1°. The agreement between the right CVA and the left CVA was found in 60 participants (72.3%) while in 23 participants the measurements were discordant and therefore they were not considered for our study.
Among the 60 participants with agreement between the measurements (defined as sample size), 45 had FHP (11 females and 34 males) with lower CVA values; the results are statistically significant both if we measure the right and left CVAs (Table 1).
A CVA comparison between subjects with FHP and non-FHP group
| FHP group (n = 45) | non-FHP group (n = 15) | Total | |||||
|---|---|---|---|---|---|---|---|
| Mean | Median | SD | Mean | Median | SD | Mean | |
| Right CVA | 48.85° | 45.36° | 3.36° | 55.72° | 54.82° | 4.54° | 48.80° |
| Left CVA | 42.35° | 41.47° | 3.89° | 53.18° | 51.37° | 3.48° | 45.68° |
There are no significant (P < 0.05) differences in all spirometry parameters between the FHP group and the non-FHP group (Table 2).
Spirometric analysis between FHP and control groups
| FHP group (n = 45) | non-FHP group (n = 15) | ||||||
|---|---|---|---|---|---|---|---|
| Units | Mean | Median | SD | Mean | Median | SD | |
| FVC | L | 99.73 | 97 | 11.83 | 99.2 | 104 | 15.53 |
| FEV1 | L | 100.62 | 101 | 9.41 | 102.67 | 106 | 20.87 |
| Tiffenau | % | 84.06 | 84 | 6.00 | 83.28 | 83.9 | 5.65 |
| PEF | L/s | 100.42 | 101 | 12.76 | 96.33 | 99 | 19.40 |
| MEF25 | L/s | 97.96 | 98 | 22.89 | 113.47 | 114 | 52.07 |
| MEF50 | L/s | 99.38 | 97 | 20.72 | 111.87 | 106 | 40.17 |
| MEF75 | L/s | 98.51 | 96 | 18.57 | 100 | 105 | 25.61 |
| FEF25–75 | L/s | 100.44 | 103 | 17.97 | 113.27 | 107 | 39.95 |
| VC | L | 96.13 | 95 | 13.15 | 94.47 | 100 | 17.15 |
| IC | L | 92.82 | 89 | 13.62 | 100.8 | 100 | 16.10 |
| MVV | L/min | 104.87 | 105 | 19.17 | 98.4 | 102 | 25.84 |
Among our sample size, 19 subjects had NDI > 9, while 41 subjects (68.3%) had NDI < 8. Moreover, even if the mean NDI values were higher in the non-FHP group compared with the FHP group, this result was not statistically significant (Table 3).
NDI scores between FHP and control groups
| FHP group (n = 45) | non-FHP group (n = 15) | |||||
|---|---|---|---|---|---|---|
| Mean | Median | SD | Mean | Median | SD | |
| NDI | 6.53 | 4 | 9.05 | 12.4 | 10 | 13.05 |
Discussion
This study investigated the effects of FHP on spirometry on a sample of 83 subjects, of whom 45 with FHP. We found no significant differences in all spirometric parameters analyzed between subjects with FHP and the non-FHP group. Moreover, no significant differences in NDI scores were found between groups.
The postural examination is a critical part of the clinical orthopaedic evaluation and different methods are available for measuring the craniocervical posture. The CVA is a widely used method for the objective measurement of FHP. In our study, the mean value of CVA in a standing position was 48.80° for the right side and 45.68° for the left side, lower than the ones found in previous studies [3, 22, 23]. This finding could be influenced by a selection bias since most of the participants were office workers.
Han et al. [10] and Kim et al. [23] reported that FVC and FEV1 levels are lower in patients with FHP compared with patients without FHP, but they reported the values of FEV1 and FVC in liters. Moreover, Kim et al. [23] reported statistically significant differences in FVC, FEV1, FEV1/FVC ratio, PEF, maximum inspiratory pressure (MIP), maximum expiratory pressure (MEP), and CVA in smartphone users [23]. For the purposes of the study, we fully met the ATS criteria and only spirometric tests of at least grade C, which represents a satisfactory score, were used for the purpose of the study. We also indexed the spirometric values, expressing them as percentages and not in liters. Spirometry is a standardized and objective test if correctly performed. Moreover, we used percentage values and not absolute values having referring to the report of GLI [20, 21] based on similar non-smoking, disease-free subjects. In these cases, spirometry data collected from a patient must be compared with data collected from biological peers who are nonsmokers with disease-free lungs because healthy lung size and function are dependent on four key variables: age, sex, height, and race [15].
Therefore, differently from most of the published literature, we found that FHP had no influence on respiratory function. Spirometric parameters in our sample size were not different between subjects with FHP and subjects without FHP. Probably the quality of spirometry exam and indexing values could be possible explanations. As a result, we hypothesize that respiratory rehabilitation is unnecessary in subjects with FHP.
The correlation between FHP and cervical disability, postulated in numerous studies [7, 10–14, 24–27], is not confirmed in our series. The cervical pain symptom and the relative cervical disability, confirmed by a score on the NDI questionnaire > 8, are not strictly correlated to the presence of FHP; among the 45 subjects who presented with FHP, only 11 of these reported suffering frequently from neck pain (NDI > 8), while the remaining 34 subjects with FHP were asymptomatic. In fact, other factors than FHP seem to have a greater influence on the symptom of neck pain, such as: female sex, advanced age, cessation of smoking, high workload and low social level [27, 28]. Only a few studies [11, 27, 28] regarding FHP and pulmonary function reported a subjective assessment of cervical disability, neither is it considered as a comparison variable between the sample under examination and the control group. It is mostly recognized as an FHP-related disorder and not considered as a possible variable of interference on lung function and muscle strength.
The strengths of this trial are: the sample size, whereas the other studies included samples made up of no more than 15–30 subjects; the heterogeneity of the sample (age 18–50, both male and female subjects), which provides more credible and repeatable results; strict adherence to the exclusion criteria in the selection of the sample; the use of widely validated and highly repeatable methods and parameters. this study excluded people with exposure to dusts or inhalents. This could be seen as a confounding factor in other studies.
Conversely, a weakness is the probable influence of occupational factors that may partially explain the high prevalence of FHP found in the population examined. In fact, it is likely that the application of some exclusion criteria related to exposure to dusts or inhalants, has helped to select a population of subjects using computer stations for a prolonged time.
Beyond this, the study offers further and promising research ideas, as the next study objectives could be represented by:
To use a more accurate imaging technique such as X-rays, in a clinical setting.
A neurophysiological assessment of the neck and respiratory muscles, testing the subjects who have FHP with a dynamometer that evaluates the strength of the extensor and flexor muscles of the neck, to understand if the subjects who develop FHP have hypotonia of these muscles.
To study subjects with cervical disability and chronic neck pain, classified on the basis of the NDI, with tests for the measurement of MIP and MEP, to evaluate the influence of neck pain more directly on the strength of the respiratory muscles. The values of MIP and MEP would seem to correlate directly with the NDI score and therefore with neck pain. In addition, the MEP values seem to be determined directly by the strength of the neck muscles [11].
Conclusions
There is no clear relationship between FHP and respiratory function indices. Moreover, no differences have been found in NDI values between subjects with FHP and subjects without FHP. Therefore, respiratory rehabilitation strategies should be focused on other parameters than FHP itself.
Abbreviations
| C7: | seventh cervical vertebra |
| CVA: | craniovertebral angle |
| FEV1: | forced expiratory volume in 1 s |
| FHP: | forward head posture |
| FVC: | forced vital capacity |
| MEF: | maximal expiratory flow |
| MEP: | maximum expiratory pressure |
| MIP: | maximum inspiratory pressure |
| NDI: | neck disability index |
| NHP: | neutral head posture |
| PEF: | peak expiratory flow |
Declarations
Author contributions
FS, SP, and AB: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. TDF, DT, A Serio, A Spinelli, and LC: Conceptualization, Investigation, Writing—original draft, Writing—review & editing. AD, GA, EK, and CMG: Validation, Writing—review & editing, Supervision. All authors read and approved the submitted version.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethical approval
This study complies with the Declaration of Helsinki.
Consent to participate
Informed consent to participate in the study was obtained from all participants.
Consent to publication
Consent to publish his photograph was obtained from the subject in the picture.
Availability of data and materials
Not applicable.
Funding
Not applicable.
Copyright
© The Author(s) 2023.